
An interesting modelling study has quantified the size of the CPE iceberg lurking under the water when CPE is only detected by clinical cultures and no active screening is done. And the CPE iceberg is larger than you may think!
An interesting modelling study has quantified the size of the CPE iceberg lurking under the water when CPE is only detected by clinical cultures and no active screening is done. And the CPE iceberg is larger than you may think!
Colistin resistance in CPE is bad news. Colistin is an older antibiotic that has been effectively brought out of retirement to tackle CPE infections. We have first-hand experience of witnessing the emergence and spread of colistin resistance in CPE – and it’s not a pretty sight. Colistin susceptibility testing is very tricky from a diagnostic laboratory viewpoint – and so I was interested in this recently published paper from colleagues at Imperial evaluating a rapid MALDI-TOF based approach to detecting colistin resistance, which looks very promising indeed.
We have been posting for a while about the emerging recognition of CPE contamination of drains in clinical settings, which seems to be fueling some CPE transmission. Until now, there’s been plenty of publications identifying the problem, but very few presenting a solution. In fact, attempts to tackle CPE contamination of drains have had moderate impact, at best. A new short study in ICHE illustrates the potential of a foaming hydrogen-peroxide based disinfectant to tackle contamination with resistant Gram-negative bacteria in drains.
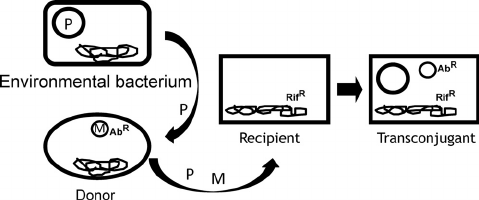
An interesting new Italian study has identified the mcr-1 gene, a plasmid-mediated colistin resistance gene, in 8% of environmental Enterobacteriaceae isolates. This suggests that environmental Enterobacteriaceae and perhaps even environmental surfaces themselves could be important reservoirs in the spread of mcr-1 and colistin resistance.
Addenbrookes hospital in Cambridge (UK) have recently performed a point prevalence survey for antibiotic resistant bacteria. None of 540 patient samples grew CPE, but 130 (24%) grew VRE. So, why no CPE but so much VRE?

A team of authors surveyed NHS acute hospitals in England to determine the approach to CPE detection, including laboratory methods. The findings provide an opportunity to compare the approach to CPE detection and prevalence nationally, identifying higher CPE prevalence in the North-West, North-East and the South-East (the region that includes London) of England. The findings also suggest that more screening for CPE would detect more carriers – and perhaps help to prevent a silent epidemic of CPE in some regions.
One of the questions that we often ask ourselves is whether carriers of CPE (and other MDR-GNR) can de-isolated. Most of the guidelines are pretty non-committal on this point due to lack of evidence. Some new guidelines from ESCMID-EUCIC address this issue head on. But, unfortunately, the answer is that de-isolation of CPE carriers, particularly over the course of a single hospitalisation, isn’t going to work because there’s no effective decolonisation method.
People have been talking in apocalyptic terms for years – probably decades – about the threat of AMR. But has this really materialised? MRSA BSIs are now rare in the UK, and C. difficile infections are rarer than they once were. But things are looking considerably gloomier in other parts of the world. For example, a frankly shocking study from a Greek ICU gives us a view of what a post-antibiotic apocalypse may look like…
Although there’s some controversy about whether or not we should apply contact precautions (by that I mean single room isolation, enhanced PPE, enhanced disinfection etc) all the time for all organisms, it would be a brave hospital to eschew contact precautions for CPE carriers. And so the question of whether and when we should ‘de-isolate’ patients with known CPE is an FAQ. And so enter a recent study in CMI comparing the spontaneous apparent loss of colonisation with various CPEs, concluding that KPC carbapenemases seem to hang around for longer than NDM carbapenemases, but both almost always last for the duration of a single hospitalisation.
The 2018 ESPAUR report was published a few weeks ago. It’s freely available for your perusal here, and packed full of juicy info. Here’s a few reflections on the report.
