“The course of an epidemic is defined by a series of key factors, some of which are poorly understood at present for COVID-19” (Roy Anderson Lancet, March 9th)
While several of the factors are obvious and come to mind immediately, others, might at this point be speculation or indiscriminate observations that need further scientific evaluation.
One of the latter category, might be the observation I would like to share in this post. One of the regions of the Netherlands that presently has one of the highest COVID-19 rates, is a region in the South of the country. To our knowledge there is only one thing unusual about that region; About ten years ago, the region was in the midst of the Dutch Q-fever epidemic. Could one of those key factors that we don’t understand and that may lead to area’s with exceptional high rates of COVID-19 be previous infectious diseases such as Q-fever, or more general a higher prevalence of previous long damage, due to infectious diseases?
Have a look at the graphs and please share your thoughts.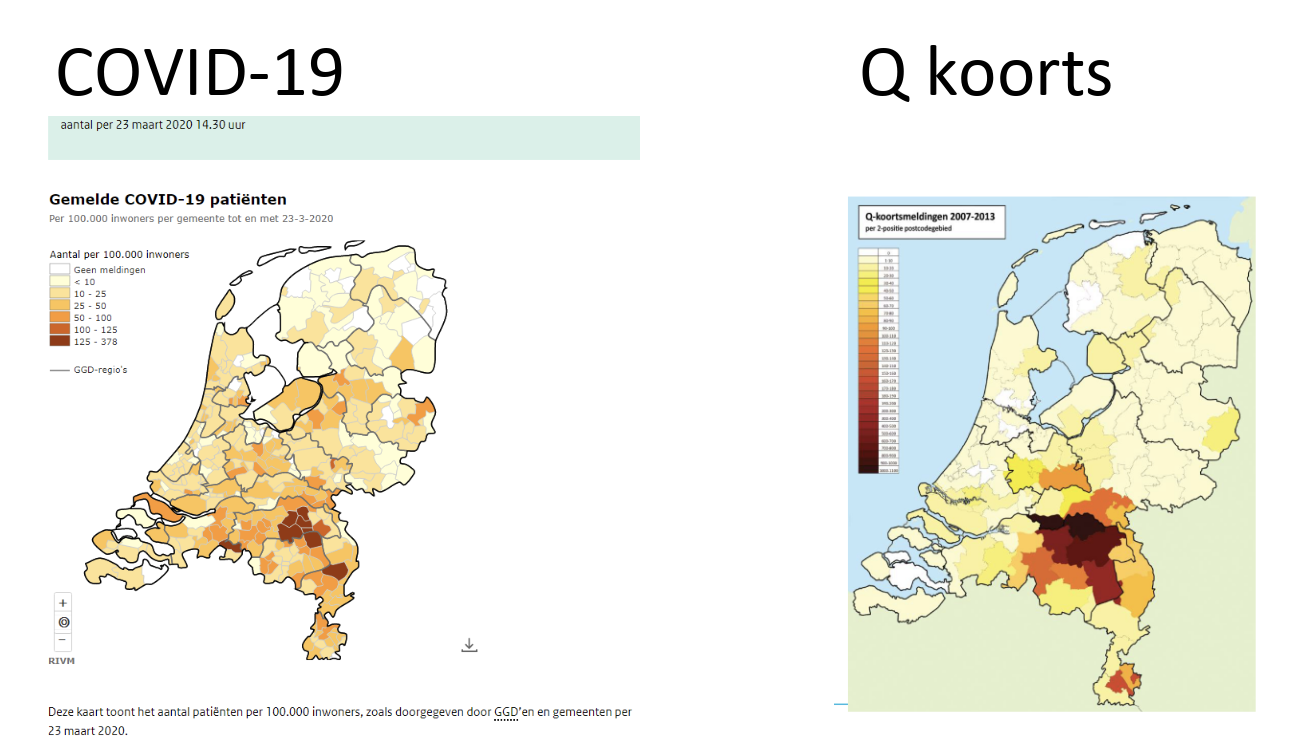
With thanks to my colleague Bert Mulder, Nijmegen





 Shortages?! Slowly, I get used to it. Basic antibiotics such as penicillins, CHX-wipes, or now, mupirocin. From what I hear we have to expect severe shortages (= no product) for the next few months. As the use of mupirocin for nasal decolonization of S. aureus (in combination with CHX skin wash) has become part of the pre-operative care for certain indications, the obvious question is: WHAT SHOULD I USE INSTEAD?
Shortages?! Slowly, I get used to it. Basic antibiotics such as penicillins, CHX-wipes, or now, mupirocin. From what I hear we have to expect severe shortages (= no product) for the next few months. As the use of mupirocin for nasal decolonization of S. aureus (in combination with CHX skin wash) has become part of the pre-operative care for certain indications, the obvious question is: WHAT SHOULD I USE INSTEAD?
 by Andreas Voss and Eli Perencevich,
by Andreas Voss and Eli Perencevich,