Ever found yourself wondering how often colonization precedes infection with MDR-GNB and VRE? A new systematic review and meta-regression in Lancet ID gives us a pretty solid answer: about 14% of MDR-GNB and 8% for VRE. This information is helpful for us to qualify the significance of acquiring these organisms in healthcare settings.
Continue readingCRE
WHO guidelines for the prevention and control of carbapenem-resistant organisms

WHO have just released some guidelines for the prevention and control of carbapenem-resistant Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aerugionsa. This guideline builds on the excellent WHO core components for IPC guidelines.
Contact Precautions for Endemic MRSA and VRE
 by Andreas Voss and Eli Perencevich,
by Andreas Voss and Eli Perencevich,
intentionally posted on “Reflections” and “Controversies” at the same time as a reaction to the JAMA Viewpoint by Morgan, Wenzel & Bearman
During the recent ICPIC 2017 and a pre-meeting think tank, the sense and non-sense of RCTs looking at various infection control measures was a major point of discussion during many sessions. Data from well-designed quasi-experimental studies, epidemiological evidence, and logic seems to vanish, whenever a new RCT is published, even if the results are not applicable to situations that are non-endemic, have higher or lower compliance with the preventive measures in question, or whether the intended measures were actually applied within the intended patient group. Some studies seem to assume that the transmission during the first days of admission are of no consequence. Others assume that given endemicity and a high patient load, the intended measures such as single-room isolation can’t be applied, even if a patient was randomized to receive those measures.
Acronyms for carbapenem-resistant bacteria (again)
I am currently involved in some research that requires a clear distinction between CPE (i.e. Enterobacteriaceae that produce a carbapenemase) and non-carbapenemase-producing CRE. Since ‘non-carbapenemease-producing carbapenem-resistant Enterobacteriaceae’ is a bit of a mouthful, I need to come up with some sort of acronym. I would appreciate your thoughts on the scheme set out below:

You can read more thoughts on acronyms for carbapenem-resistant bacteria in a previous post here.
Antibiotic Awareness: background and links
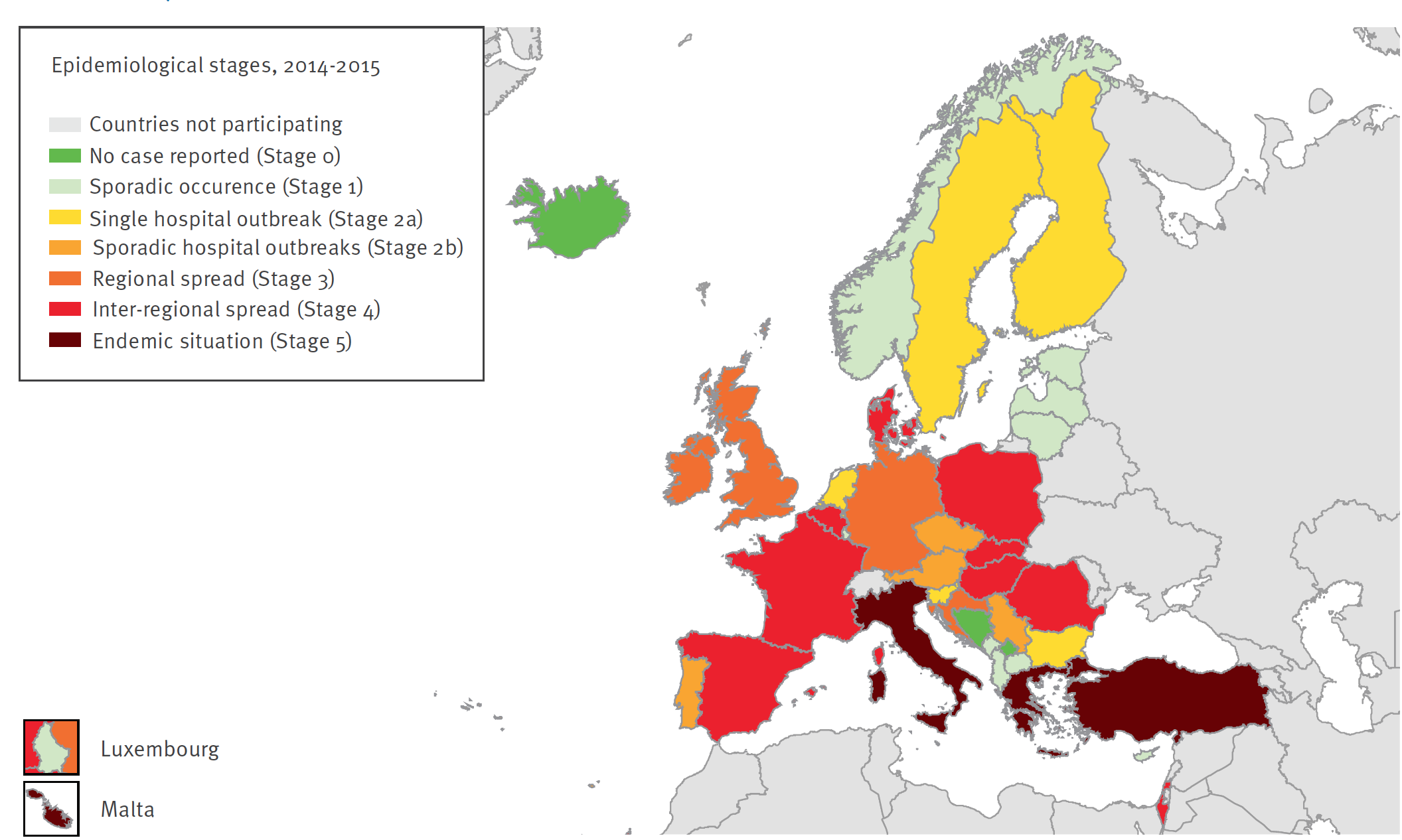
European Survey of Carbapenemase-Producing Enterobacteriaceae (EuSCAPE) project
The EuSCAPE project aimed to improve understanding of the occurrence and spread of CPE. LINK
About European Antibiotic Awareness Day
European Antibiotic Awareness Day is a European health initiative coordinated by ECDC which aims to provide a platform and support for national campaigns on the prudent use of antibiotics. Each year across Europe, the European Antibiotic Awareness Day is marked by national campaigns on the prudent use of antibiotics during the week of 18 November. Prudent use means only using antibiotics when they are needed, with the correct dose, dosage intervals and duration of the course. Follow the European Antibiotic Awareness Day: #EAAD. http://antibiotic.ecdc.europa.eu
About World Antibiotic Awareness Week
The World Health Organization is leading a global campaign for the first World Antibiotic Awareness Week with the slogan “Antibiotics: Handle with Care”. The campaign calls on individuals, governments and health and agriculture professionals to take action to address this urgent health problem. The first World Antibiotic Awareness Week will take place on 16-22 November. Follow the World Antibiotic Awareness Week: #AntibioticResistance. www.who.int/drugresistance.
Continue reading
CRE -> CPE

I have thought a lot (probably too much) about the best way to describe the issue of carbapenem resistance in Enterobacteriaceae. I decided ages ago that CRE (a la the CDC) is the way to go as a generic term to describe the problem. But the more I think about it, the more I am coming around to the idea that CPE (a la PHE) is better. And here’s why:
- The real issue from a clinical and infection control viewpoint is CPE. Enterobacteriaceae that are resistant to carbapenems by means other than an acquired carbapenemase (i.e. CRE that are not carbapenemase producers) are important, but they don’t seem to have the same capacity to spread as carbapenemase producers.
- It’s a really confusing situation in terms of terminology. From the “end user” staff member on the front line and patient, all that really counts is whether it is a CPE or not. It’s really rather confusing to tell a patient that the have a “CRE that is also a carbapenemase producer” – easier just to say “you have a CPE”. (I accept that you will also need to tell a patient if they have a CRE that is not a carbapenemase producer – but I think this way around is easier.)
- CPE is already en vogue in the UK (mainly due to the PHE Toolkit) so using any other term risks confusion at the time of patient transfer. (Clearly, this point is reversed if you are working in the US!)
I still think that “CRO/CPO” is not the way to go, given the gulf in epidemiology between the Enterobacteriaceae and the non-fermenters (although, sometimes, begrudgingly, you have to go there). What I mean by this is that you will sometimes detect a carbapenemase gene from a PCR but don’t yet know whether it is from a non-fermenter or Enterobacteriaceae species. In this circumstance, this has to go down as a ‘CPO’.
So, there you have it, a personal U-turn. CRE -> CPE. But I wonder whether CDC and PHE and the international community will ever agree a common term…
Reconsidering the burden of CRE screening

Shortly after the PHE Toolkit was published, I blogged some crude sums to size the burden of CRE admission screening a la Toolkit. I’m pleased to report that colleagues at Imperial have done a much better job of this, published in a letter in the Journal of Infection. The study provides some evidence that the recommendation in the PHE CRE Toolkit to perform pre-emptive isolation of suspected carriers whilst obtaining three negative screens is simply not feasible. The team then compare an alternate strategy – of applying the Tookit triggers to admissions to high risk specialties only (intensive care, nephrology, cardiothoracic surgery, neurosurgery and oncology).
We need to work together to reduce CRE and other pathogens
Some fascinating modelling from the CDC Vital Signs programme suggests that a co-ordinated, multi-facilitiy approach will be much more effective than each hospital doing its own prevention interventions.
The team first estimated the burden of key infections in the US: CRE, multi-resistant P. aeruginosa, invasive MRSA and CDI combined were responsible for 310,000 infections in 2011, which would increase 10% to 340,000 over 5 years. However, with an ‘aggressive’ national intervention, this could be reduced to below 200,000 by 2019. It would be a huge undertaking to implement and co-ordinate a national campaign in the US, where there is so much heterogeneity in the way that hospitals are structured and funded. But if anybody can do it, the CDC can!
Is CRE lurking in nursing homes?

They say that things come in threes, so following hot on the heels of blogs about MRSA and other MDROs in nursing homes, I was struck by a recent outbreak report of CRE associated with nursing homes the Netherlands.
Following the admission of a patient from a Greek ICU, a nosocomial transmission of CRE (ST258 KPC K. pneumoniae) occurred. By the way, this occurred despite the hospital recognising the risk of CRE at the time of admission from the Greek ICU, perform an admission screening and implementing pre-emptive contact precautions. Then the index patient was transferred to a nursing home, where subsequent transmission occurred to four other patients.
CRE winging its way around the world

CRE are known to be adept at hitchhiking around the world, hence the focus on cross-border transmission in Europe. A startling example of this comes in a report from Poland result from the terrorist shootings in Tunisia. Two Polish nationals seriously injured in the shootings were repatriated following a 10-day stay in a hospital in Tunis, Tunisia. A grand total of four CREs were identified from the two patients!
Three of these were identified at the time of admission, so almost certainly originated in Tunisia. The fourth CRE was identified 10 days after repatriation to Poland. The authors suggest that the most likely explanation for this is poor sensitivity of admission screening. I venture, however, that it’s more likely due to in-hospital transmission in Poland, since the two patients were treated by the same staff.
Nonetheless, the most troublesome finding here is that at least three separate CREs were imported into Poland by just two patients. Can anybody find me a paper on the prevalence and epidemiology of CRE in Tunisia? No? Thought not. The implication here is that CRE is already far more established than feared in Tunisia and many other parts of the world!
Image: Aeroplane.
