
WHO have just released some guidelines for the prevention and control of carbapenem-resistant Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aerugionsa. This guideline builds on the excellent WHO core components for IPC guidelines.
I had the privilege of being on the working group that formulated the UK guidelines on MDR-GNR, so I understand fully the challenges for the working group behind this useful addition. As a guideline writing group, perhaps the first question to answer is what will be the scope of the guidelines? In this case, CPE only? All antibiotic-resistant Gram-negatives? All carbapnem-resistant organisms? Or some other antibiotic / organism combination? For reasons that I understand, but don’t agree with, these guidelines focus on carbapenem-resistant organisms of multiple species. (My own view is that you’d be better to either cover all antibiotic-resistant Gram-negative bacteria – not just carbapenem-resistant ones – or to focus specifically on CPE.) Incidentally, the guideline development group is a truly international bunch, which is great to see (although it a little disappointed not to see anybody form the UK included in the group).
Another important question is acronyms. WHO decide to use a number of different / non-standing acronyms: CRE (ok, although would prefer CPE or CP-CRE), CRAB (just about ok, but could be mistaken for a crustacean!), and CRPsA (really??). This is more than just semantics about acronyms though – by linking together these three organism-groups (CRE, CRAB, and CRPsA), there could be an assumption, especially among the uninitiated, that the epidemiology of these organism-groups is similar, which it isn’t. Similarly, there may be an assumption that what works to control CRE will also work to control CRAB, which is won’t! So, whilst I don’t object to focussing on carbapenem-resistance, I’m not sure that lumping together these disparate organism-groups in a set of guidelines is the best approach.
And so to the recommendations; the guidelines include eight of them:
- Recommendation 1: Implementation of multimodal infection prevention and control strategies. I suppose another way of saying this would be intervention bundles. I can’t help but thinking that this stems from the poor quality of the evidence base: since we don’t really know which interventions are effective, we have to recommend the ‘kitchen sink’ approach!
- Recommendation 2: Importance of hand hygiene compliance for the control of CRE-CRAB-CRPsA. Nobody is going to argue with this one!!
- Recommendation 3: Surveillance of CRE-CRAB-CRPsA infection and surveillance cultures for asymptomatic CRE colonization. Worth dwelling for a moment on how tricky CRE (and especially CPE) is to detect. We have a hugely well-funded lab (by international standards) and still get caught out occasionally by CRE/CPE; implementing carabapenem-resistance surveillance in a poorly funded lab setting is a real challenge! The guidelines recommend screening for CRE in all settings, guided by local epidemiology and risk assessment, but no screening for CRAB / CRPsA, which is different to the other analogous international guidelines (see Figure 1 below). There is a short comment about possible resistance to CRE screening for various reasons: the answer to this (in my view) is education education education!
- Recommendation 4: Contact precautions. The guidelines use an interesting definition of contact precautions ((1) appropriate patient placement; (2) use of personal protective equipment, including gloves and gowns; (3) limiting transport and movement of patients; (4) use of disposable or dedicated patient-care equipment; and (5) prioritizing cleaning and disinfection of patient rooms). The specific reference to gloves and gowns won’t make everybody happy in the UK, where aprons are generally favoured! There is no specific reference about cohorting staff, or staff screening (in contrast to other guidelines – see Figure 1 below).
- Recommendation 5: Patient isolation. The WHO guidelines also include a recommendation around patient cohorting in this section; patient with known CRE / CRAB / CRPsA should be isolated in single rooms or cohorted together if that’s not possible.
- Recommendation 6: Environmental cleaning. The guidelines make reference to the use of hypochorite as an effective agent for disinfection, and that sometimes clinical areas will need to be emptied to facilitate thorough disinfection. There’s a somewhat disparaging reference to hydrogen peroxide, which ‘…while seemingly effective, can be disruptive to hospital workflow and bed utilization given the time and equipment required for their use.’ And no mention of UVC. My own view is that despite these drawbacks, hydrogen peroxide or UVC should be considered for terminal disinfection following carbapenem-resistant organisms. But I understand that these technologies may be further down the ‘to-implement’ list in a LMIC setting, where there may well be bigger environmental cleaning and disinfection fish to fry, so to speak.
- Recommendation 7: Surveillance cultures of the environment for CRE-CRAB-CRPsA colonization/contamination. The guidelines recommend taking cultures of the environment only when epidemiologically indicated (usually during outbreaks), and only then for CRAB.
- Recommendation 8: Monitoring, auditing and feedback. Vital for the effective implementation of any guidelines. Some recommendations will be easier to monitor than others – how would you know if your lab is missing some CRE for example? But we should certainly harvest the low-hanging fruit here (e.g. accurate measurement of hand hygiene compliance).
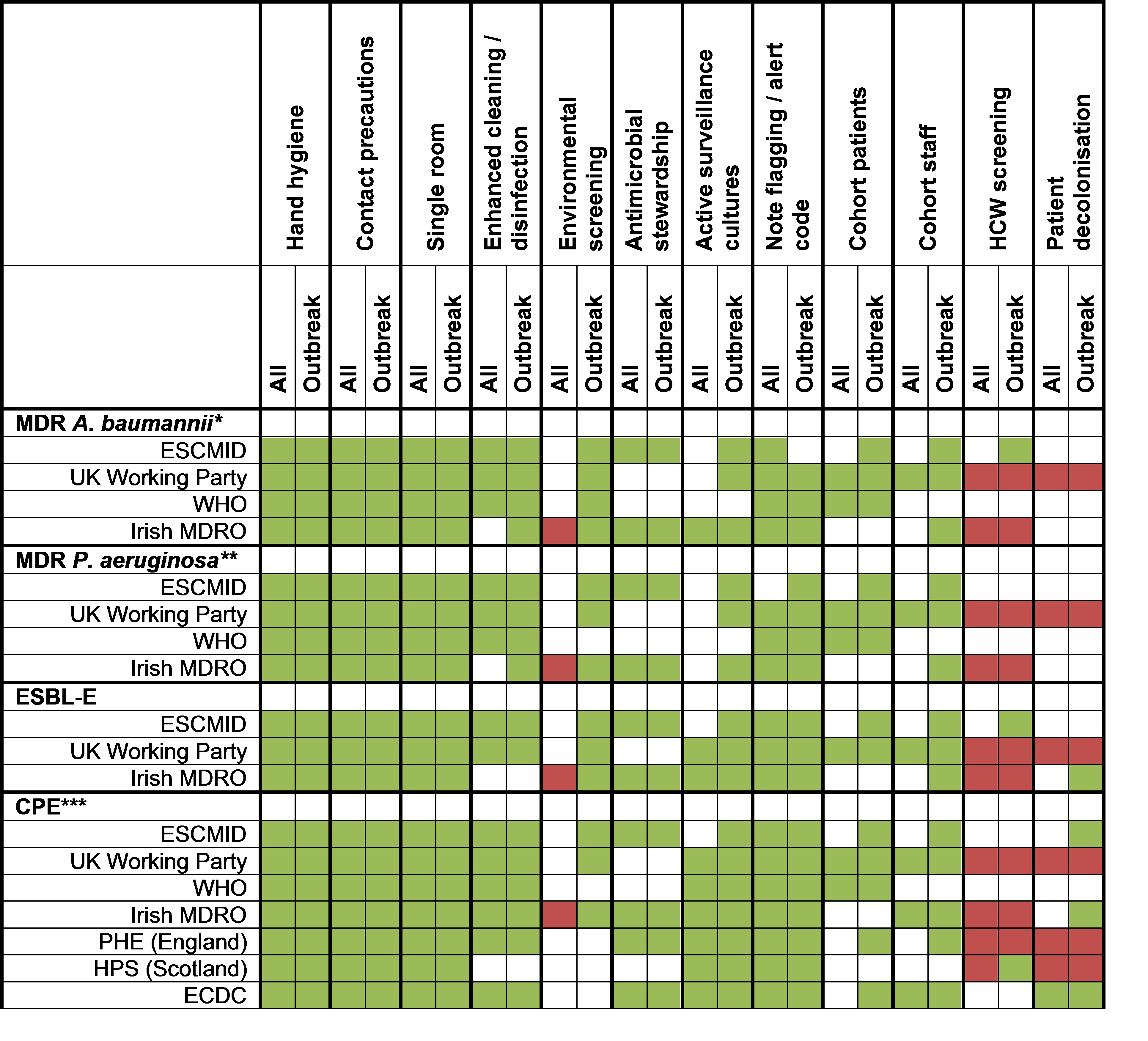
A year or two ago I wrote a review for CMI comparing the various guidelines available for MDR-GNR, which I’ve updated below to include these latest WHO guidelines and the UK Working Party guidelines (which were published after the review – there’s a story about this that I’ll tell you over a beer sometime).
Figure 1: Overview of recommendations for MDR-GNR. * CRAB in WHO guidelines. ** CRPsA in WHO. ***Multidrug-resistant Klebsiella pneumoniae in the ESCMID and CRE is WHO; green squares = recommended; red squares = not recommended; white squares = not mentioned or no recommendation.
As usual when reviewing this sort of guideline, I am struck by the disparity between strong recommendations underpinned by weak, very weak, or non-existent evidence. This is far from ideal – and we need to work together to improve the evidence-base around this vitally important healthcare issue. I was rather disappointed not to see more specific reference to antimicrobial stewardship as a key intervention to tackle carbapenem-resistance, especially in light of WHO’s recent rhetoric around integrated IPC/AMR programmes!
All in all though, some more useful, carefully researched, and well-written guidelines that should help us to prevent the spread of carbapenem-resistant organisms more effectively.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

Tom Gottlieb has pointed me in the direction of some recently published Aussie CPE prevention and control guidelines (which I’ll review after the Ashes – the result may influence my slant) https://www.safetyandquality.gov.au/our-work/healthcare-associated-infection/cpe-guide/
LikeLike
Not a lot! We frequently see a +-+ pattern over weeks and months!
LikeLike