Colistin resistance in CPE is bad news. Colistin is an older antibiotic that has been effectively brought out of retirement to tackle CPE infections. We have first-hand experience of witnessing the emergence and spread of colistin resistance in CPE – and it’s not a pretty sight. Colistin susceptibility testing is very tricky from a diagnostic laboratory viewpoint – and so I was interested in this recently published paper from colleagues at Imperial evaluating a rapid MALDI-TOF based approach to detecting colistin resistance, which looks very promising indeed.
colistin
Mcr-1 plasmid-mediated colistin resistance genes in environmental Enterobacteriaceae
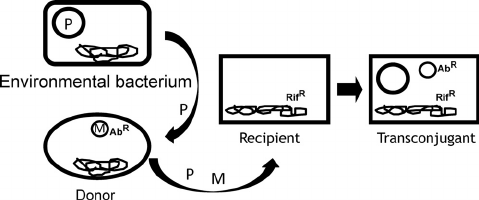
An interesting new Italian study has identified the mcr-1 gene, a plasmid-mediated colistin resistance gene, in 8% of environmental Enterobacteriaceae isolates. This suggests that environmental Enterobacteriaceae and perhaps even environmental surfaces themselves could be important reservoirs in the spread of mcr-1 and colistin resistance.
Mutational colistin resistance in CPE is the clear and present danger, not plasmid-mediated mcr genes
There has been a lot of concern in scientific journals and the mainstream media about colistin resistance in Enterobacteriaceae caused by plasmid-mediated resistance genes (the mcr genes). However, an article published today by our group suggests that mutational colistin resistance rather than plasmid-mediated mcr genes is a more pressing clinical threat.
Colistin resistance in CPE: an emerging threat

I am becoming increasingly interested in colistin resistance in CPE, not least because of this work that we will be presenting on colistin resistance in CPE at ECCMID in a few months time. I have been brushing up on how colistin resistance occurs in CPE, and why it is important, so thought I’d share my findings. I started with a pubmed search for “colistin resistance mechanism” on 12/02/16 and this is what I found (85 hits from the initial search):
Colisin
Colistin is an old class (discovered during WWII) of cationic antibiotic. Colistin (polymyxin E) is a polypeptide bactericidal agent and is one of the two clinically available forms of polymyxin agents (polymyxin B and polymyxin E). Colistin interacts with lipopolysaccharide in the outer membrane, resulting in a leaky and ultimately dead bacterial cell.1 Issues with presumed nephrotoxicity have kept colistin very much on the top shelf, but the emergence of CPE has brought colistin down a shelf or two – and we are learning that the nephrotoxicity tradionally associated with colisin may not be so bad afterall.1
Transmissible colistin resistance – made in China

The emergence of CPE (and carbapenem-resistance in other Gram-negative bacteria) has forced us to reach to the dusty old antibiotic shelf to revive the clinical use of older agents with activity against Gram-negative bacteria, principally colistin. Colistin isn’t perfect by any means – it has poor tissue penetration compared with the carbapenems, and is associated with nephrotoxicity (although the high levels of nephrotoxicity in the older medical literature has not been reported due to better management of the drug). Furthermore, resistance has already been reported. To date – this has been mutational resistance, which does not have the capacity to spread horizontally. It was only a matter of time before a colistin resistance gene mobilised.
A postcard from São Paulo, Brazil: thank goodness for the NHS
 I recently had the opportunity to spend a week in São Paulo, Brazil, to meet with some infection control and infectious diseases folks. I came away feeling pretty disturbed and very grateful for the NHS.
I recently had the opportunity to spend a week in São Paulo, Brazil, to meet with some infection control and infectious diseases folks. I came away feeling pretty disturbed and very grateful for the NHS.
Brazil is a massive country, with almost 200m inhabitants. São Paulo is Brazil’s largest city, with more than 20m inhabitants making it the 7th largest city in the world. I have lived in London and close to New York, and spent quite some time in Tokyo but nothing comes close to the traffic in São Paulo. It took me 3 hours to travel the 30km from the airport to the hotel, not because it was the middle of the rush hour or because there was a problem, just because the volume of traffic is too big for the infrastructure to handle.
Brazil has around 7000 hospitals; 70% are private with a healthcare insurance system for those who can afford it. The public hospitals are the only option for those who cannot afford healthcare insurance. I visited a number of public and private hospitals and was struck by the following:
- Rates of antibiotic resistance are eye-wateringly high. Around 40% of healthcare-associated Klebsiella pneuomoniae are carbapenem-resistant and of these, around 20% are colistin-resistant. More than 50% of K. pneumoniae produce ESBLs. The situation with Acinetobacter baumannii is even worse, with >80% resistant to carbapenems. Whilst there is usually some treatment option left, pan-drug resistant Gram-negative bacteria are a daily reality on the ICUs. To top it off, around 60% of S. aureus are MRSA, 80% of E. faecium are VRE and C. difficile is chronically under-reported due to lack of testing infrastructure and limited awareness about sending specimens. There’s an excellent 2011 review on antibiotic resistance in Brazil here, although a lot has happened since 2011.
- The public hospitals are chronically overcrowded. This is best illustrated by a quick visit to the Emergency Department, where patients on stretchers line the corridors as far as the eye can see. These patients usually stay for days, not hours. The problem is so endemic that ICUs have been established in the ED. The wards are crowded too, with very small distances between beds. Plus, there are not enough staff to cover their beds, especially during nights and weekends. Following one meeting at a very large public hospital (2000 beds), we literally could not leave the building due to the sheer volume of patients trying to get in. Just like the roads, the volume of patients is too high for the infrastructure to handle.
- The contrast between public and private hospitals is stark. Instead of being met by patients on stretchers when you arrive at public hospitals, you’re met by glass fronted healthcare insurance offices.
So, what can be done? The various strategies to curb the growing threat of antibiotic resistance are as relevant in Brazil as elsewhere: prevention is better than cure; reduce antibiotic use; improve accurate and timely diagnosis; perform surveillance for action; embrace novel solutions; highlight the financial burden; and develop new antibiotics. Some progress has been made, for example, antibiotics are no longer available without prescription over-the-counter. The commitment and enthusiasm of the infection control and infectious diseases folks that I have met here is inspiring. However, they are limited by poor healthcare infrastructure, virtually no investment in microbiology laboratory facilities, lack of national reporting, the widespread availability of poor-quality antibiotics and extensive use of antibiotics in the veterinary sector, which makes progress difficult.
Next time you have the misfortune of visiting an Accident & Emergency Department in an NHS hospital, rather than moan if you have to wait a few hours to access world-leading healthcare free at the point of care, instead be thankful for the NHS.
Photo credit: Fred Inklaar.
Is treating surfaces rather than patients with colistin a good idea?
 Antimicrobial resistance is a worldwide problem and the emergence of multi-drug resistant (MDR) bacteria and the lack of therapeutic options have led to the revival of old antibiotics such as colistin.1 This antibiotic is now considered as a “last line” antibiotic used to treat infection with MDR strains especially those cause by Gram-negative pathogens.2 Unfortunately, resistance to colistin has already been documented among a number of problematic pathogens such as Pseudomonas aeruginosa, Acinetobacter baumannii and Klebsiella pneumoniae, although the exact mechanism of resistance is not yet well defined.3
Antimicrobial resistance is a worldwide problem and the emergence of multi-drug resistant (MDR) bacteria and the lack of therapeutic options have led to the revival of old antibiotics such as colistin.1 This antibiotic is now considered as a “last line” antibiotic used to treat infection with MDR strains especially those cause by Gram-negative pathogens.2 Unfortunately, resistance to colistin has already been documented among a number of problematic pathogens such as Pseudomonas aeruginosa, Acinetobacter baumannii and Klebsiella pneumoniae, although the exact mechanism of resistance is not yet well defined.3
Within this context, I was surprised to come across a study4 presented at the 23nd European Congress of Clinical Microbiology and Infectious Diseases (ECCMID) conference held in Berlin in April 2013, by a Portuguese group aimed at covalently immobilizing colistin on biomaterials to prevent biomaterial-associated infection.
The use of antimicrobial materials and materials coated or impregnated with antimicrobial agents in healthcare settings is a flourishing field of research. This is driven by an increased recognition of the role of environmental surfaces in the transmission of nosocomial pathogens5 as well as the age old problem of bacterial colonisation of indwelling medical devices.6 With few exceptions, such materials have yet to be proven effective in reducing infection in practice. In addition, the possibility of the development of resistance to the active agents within these materials and surfaces has not yet been well investigated.
The Portuguese study,4 successfully covalently immobilized colistin onto a polycarbonate surface using a polydopamine dip-coating methodology. They used two strains of P. aeruginosa to test for the ability of the bacteria to attach to these colistin coated surfaces and the antimicrobial activity of these surfaces. The results showed that colistin coated surfaces had no effect on bacterial attachment and that the majority (but not all) of the bacterial cells were killed. So, some cells were still viable after 24 hr incubation on the colistin coated surfaces. The concentration of colistin used was not reported, but it is clearly not sufficient to inactivate all the cells on the surfaces which can potentially lead to the development of resistance to the drug, especially in a versatile organism such as P. aeruginosa.
I believe that in an era of MDR and pan-resistant strains and virtually untreatable bacterial infections, the idea of using one of our last line antibiotics to coat biomedical surfaces potentially breading colistin and other antimicrobial resistant strains is the last thing the healthcare community needs.
References
- Bergen PJ, Landersdorfer CB, Lee HJ, Li J, Nation RL. ‘Old’ antibiotics for emerging multidrug-resistant bacteria.Curr Opin Infect Dis. 2012 Dec;25(6):626-33
- Biswas S, Brunel JM, Dubus JC, Reynaud-Gaubert M, Rolain JM. Colistin: an update on the antibiotic of the 21st century. Expert Rev Anti Infect Ther. 2012 Aug;10(8):917-34.
- Lim LM, Ly N, Anderson D, Yang JC, Macander L, Jarkowski A 3rd, Forrest A, Bulitta JB, Tsuji BT. Resurgence of colistin: a review of resistance, toxicity, pharmacodynamics, and dosing. Pharmacotherapy. 2010 Dec;30(12):1279-91
- Alves D, Lopes S, Pereira MO. A colistin coating to prevent biomaterial-associated infections. ECCMID. 2013. Berlin. Abstract P1105.
- Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect Control Hosp Epidemiol. 2011 Jul;32(7):687-99
- Nicolle LE. Urinary catheter-associated infections. Infect Dis Clin North Am. 2012 Mar;26(1):13-27.
