Colistin resistance in CPE is bad news. Colistin is an older antibiotic that has been effectively brought out of retirement to tackle CPE infections. We have first-hand experience of witnessing the emergence and spread of colistin resistance in CPE – and it’s not a pretty sight. Colistin susceptibility testing is very tricky from a diagnostic laboratory viewpoint – and so I was interested in this recently published paper from colleagues at Imperial evaluating a rapid MALDI-TOF based approach to detecting colistin resistance, which looks very promising indeed.
Colistin resistance ‘hit the big time’ with the discovery of the mcr-1 gene in China in 2015. The concern was that this plasmid-mediated gene (and it’s cousins mcr-2, 3, 4 etc) will spread rapidly across the globe and make colistin redundant. Whilst the prevalence of mcr genes in CPE is indeed very high in some parts of the world, this is not true everywhere – a recent prevalence survey in the UK found that mcr genes were rare (<0.1%, 15/24,000 isolates). Conversely, during an outbreak of CPE in London, chromosomal colistin resistance was detected in two thirds of isolates and spread rapidly, causing us to conclude that chromosomal colistin resistance is a bigger threat than plasmid mediated resistance in our setting. Another aspect of this outbreak investigation is that, worryingly, our local testing suggested that only 24% of the 38 isolates were colistin resistant. Even more concerning is that the gold standard phenotypic method used by the reference laboratory has been superseded, so may not have been that golden as a standard after all!
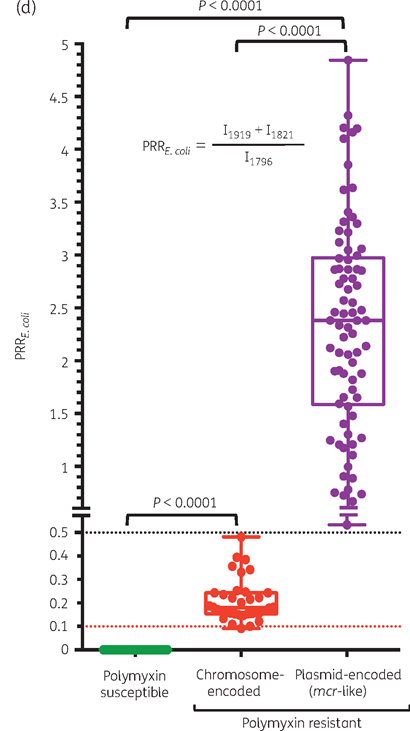
So, as you can see, colistin resistance detection is a major clinical threat and perhaps and even bigger diagnostic challenge (see recent review here from a diagnostic viewpoint). This has prompted a host of new approaches to detecting colistin resistance. One such innovation is the use of MALDI-TOF to detect the metabolites of colistin resistance. The study investigated several panels of E. coli from library collections and clinical isolates. The method was very effective at classifying the isolates as susceptible, resistant by a plasmid-mediated mechanism, or resistant by a chromosomal mechanism (see Figure 1).
Figure 1: Classification of isolates into susceptible or resistant, by mechanism
The method is very promising because it offers rapid, high-throughput, low cost screening for colistin resistance. It has a major benefit over genomic methods, which don’t tell us whether or not a gene is being expressed. It also has the added benefit of distinguishing between plasmid and chromosomal mechanisms. However, it only offers a ‘binary’ answer (i.e. colistin resistant or not) – it doesn’t tell us anything about the level of susceptibility. And it won’t be able to detect unusual or new mechanisms of resistance.
There’s still a way to go before this method is ready for the routine clinical microbiology laboratory – but I’m hopeful that it could provide a very useful tool in detecting colistin resistant bacteria.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
