I posted recently on the potential risk of CPE contamination of sinks, drains, and hospital wastewater. The question in my mind then was whether contamination is a smoking gun or innocent bystander regarding CPE transmission? What we really need is an intervention to show that better management of sinks and drains results in reduce CPE transmission. And now, we have one! The findings suggest that attempts to control CPE will go down the drain if we don’t intervene to improvement the management of sinks and drains.
The study centred around the impact of installing covers for hoppers (a toilet like waste disposal unit) and sink trap heater/vibration devices. The hopper covers were to prevent aerosolisation of CPE when the hoppers were flushed, and the sink trap heaters/vibration devices were to heat-sanitise the drain and dislodge the formation of biofilm. Since the hoppers were present in rooms in all ICUs, the study focussed on these units. The sink trap heater/vibration devices were only installed on one of the ICUs, which had the highest rate of CPE prior to the intervention. Only patients exposed to a hopper unit were included in the study. The outcome focussed on KPC-producing Enterobacteriaceae, rather than a specific bug-gene combo.
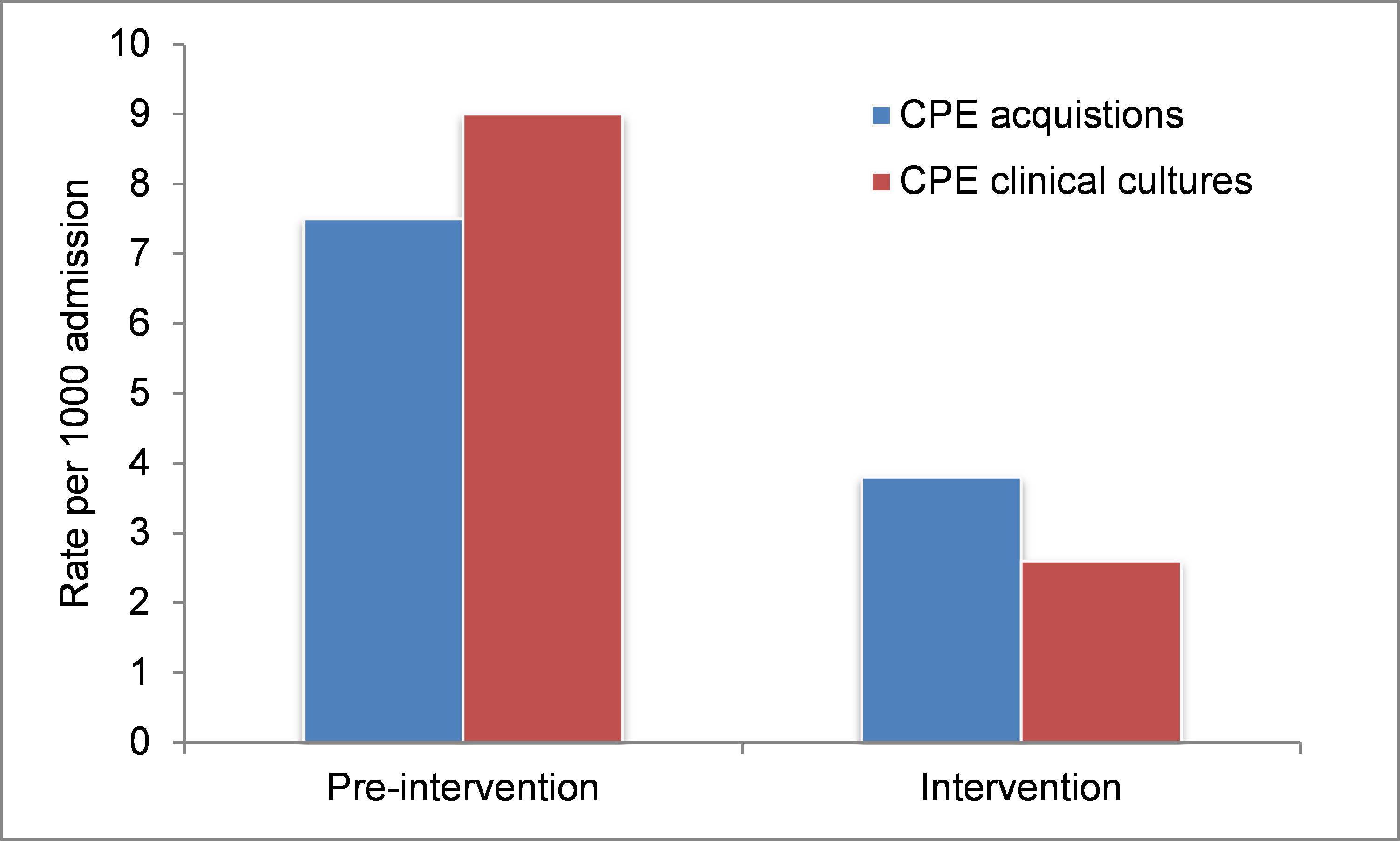
The study was a before-after design, with an 18 month pre-intervention phase, a 3 month installation phase (of the hopper covers and sink trap heater/vibration devices), and an 18 month intervention phase. The results were spectacular: 56 new Klebsiella pneumoniae carbapenemase–producing organism (I’ll call them CPEs for simplicity here) acquisitions in the pre-intervention vs. only 30 in the intervention. This equated to an incidence rate ratio of 0.51; effectively a halving of new CPE acquisitions (see figure below)! Clinical cultures also dropped dramatically and significantly (reduced by two thirds). I was surprised to see that the rate of clinical cultures was higher than the rate of acquisitions in the pre-intervention phase. Interestingly, the longer you spent close to a hopper was a significant risk for acquisition in the pre-intervention phase, but not during the intervention phase. There was even a reduction of CPE acquisition for patients not exposed to the hoppers over the same period, perhaps suggesting some sort of halo effect.
Figure: The rate of CPE acquisition and CPE clinical cultures before and during the intervention.
These dramatic clinical findings are supported by extensive environmental sampling. A whopping 75% of hoppers and 80% of sink traps were contaminated with CPE prior to the intervention, with 31% of the hoppers contaminated with multiple CPEs. Worth nothing here that many of the CPE cultured from the hoppers was in Aeromonas species, which I suspect would be a rare cause of human infection or colonisation, but perhaps acted as a sink (!) for the KPC gene. During the intervention phase, only 5% of sink traps were contaminated with CPE – quite a drop from 80%! (Oddly, there is no mention of sampling hoppers during the intervention – not sure why this is.)
I like the fact that the study team audited compliance with the intervention (Martin will be especially pleased). The worry is that when this intervention leaves the study setting, the hopper lids will be closed once in a blue moon, and the sink trap devices won’t be working most of the time and nobody will notice! This certainly wasn’t the case during the study. It’s useful to see the cost of the intervention highlighted in the discussion: $48,000 for the hopper covers, and $50,000 for the sink trap heater/vibration devices. So, not exactly a low-cost intervention, but if the clinical impact is real, you’d see your money back in no time.
So, are we really left to conclude that more than 50% of CPE acquisition events are directly or indirectly linked to contaminated hoppers and sink drains? This is what the study suggests, and the fact that this is an intervention study reinforces that. But since the design is before-after without an extant control unit or randomisation, we can’t fully understand other factors that may have influenced these dramatic reductions. On this point, it’s important to highlight that the routine disinfectant was changed from a QAC to a peracetic acid based disinfectant in month 13 other intervention period, which may have contributed to the overall reduction. Still, I am left concluding from these findings that contaminated sinks and drains may be a vitally important component of CPE transmission dynamics.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
