Following on from Jude’s post earlier in the week and subsequent Journal Club discussion on the role of patients in hand hygiene, I thought I’d follow suit by look at a qualitative study about patient views on IV vs. oral antibiotics for S. aureus BSI. The short answer is that patients preferred the oral choice, even though this was view as more complicated and less effective than IV antibiotics!
Continue readingBSI
Delving into Candida species bloodstream infections
To get us in the mood for Dr Nneoma Okeke’s Journal Club tomorrow (register here!), I’ve been reading the paper that will be covered. Over the past two decades, a huge population-based study in Queensland, Australia sheds light on the evolving landscape of Candida and Candida-like species bloodstream infections. This analysis, including 2,586 episodes across 2,420 patients, reveals critical trends in species prevalence, resistance patterns, gender differences, and clinical outcomes that have significant implications for healthcare practices.
Continue readingS. aureus and SSI: all roads point to nasal colonisation
I’ve written this post in preparation for tomorrow’s Journal Club, which will be about this paper on S. aureus colonisation and SSI (register here). Having not written or reviewed much on S. aureus for quite a while, I’m reading my second S. aureus paper in two weeks, following last week’s blog on a paper from the Healthcare Infection Society special on “MRSA: the enduring foe“!
Continue readingHCAI and AMR point prevalence from Ukraine
JHI have just published an interesting point prevalence HCAI and AMR study from Ukraine. Headlines are that rates of both HCAI and AMR are higher than you’d hope to see, especially with rates of resistant to carbapenems in Gram-negative bacteria and meticillin in S. aureus.
Continue readingCounting the cost of HCAI
A Journal of Hospital Infection special edition focusses on the cost of HCAI, publishing the results of the Scottish from the Evaluation of Cost of Nosocomial Infection (ECONI) Study.
Continue readingESPAUR 2019: a snazzy facelift
The 2019 edition of the ESPAUR report has recently been published, including data up to and including 2018. The report is an excellent read – here’s a few summary points.
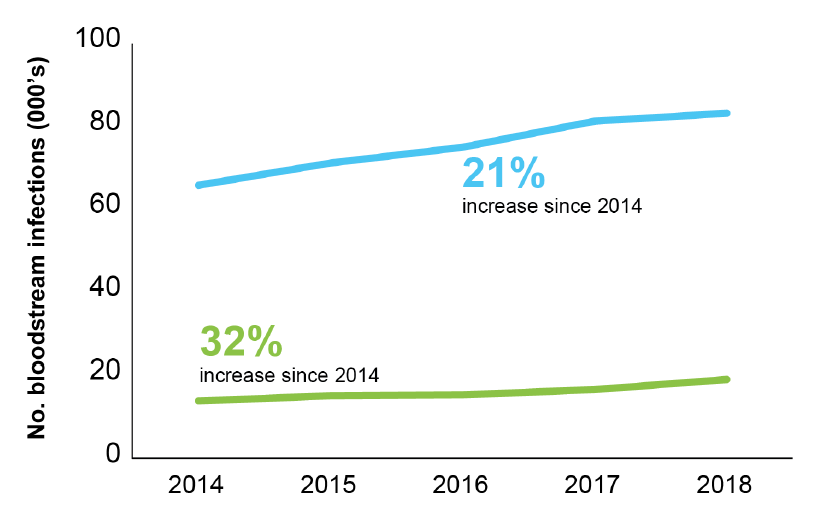
- There’s a series of lovely infographics at the start of the report. I gave myself a challenge: to select the one infographic that told the story of the report. I toyed with the one about a small but increasing number of CPE BSIs (aghhhhh!), and the stark grave-stone themed image of mortality related to carbapenemase-producers, but ended up with this one: alarmingly, the rate of BSI for the seven priority bacterial pathogens rose 22% between 2014 and 2018 to 145 per 100,000 population. (Around half of these were coli). And there’s a certain inexorability about the antimicrobial resistance trends included in this report, with a 32% increase in AMR BSIs comparing 2014 to 2018.
Figure: Trends in BSIs (blue line) and AMR BSIs (green line).
- There were more than 60k antibiotic resistant severe infections in 2018, <150 per day.
- Confirmed CPEs have topped 4k (but this is a gross underestimate of true prevalence). The report makes the case that the rarity of CPE BSIs (142 reported nationally) represents a success of prevention. This is probably true if we compare across the pond and towards the southern reaches of Europe. But difficult to be sure without a control (i.e. what would have happened without the national initiatives etc)? Also, reporting of CPE BSIs to PHE is voluntary and not mandatory, so there will be some degree of under-reporting.
- Related to this, only 50% of diagnostic labs have introduced methods to detect CPE locally. Which links closely with the change in surveillance system for CPEs going forwards – rather than manual voluntary reporting, locally confirmed CPEs will be reported automatically to PHE. However, if only 50% of diagnostic labs have appropriate methods, we’ll still end up under-reporting (but it will be more a more accurate picture than the current process provides).
- 30 day all-cause mortality of invasive CPE infections is 24% (along with the arresting gravestone-themed infographic)! Not sure how helpful it is to make a big point based on unadjusted mortality data…
- Overall consumption of antibiotics continues to decline. Consumption fell from 20 to 18 DDDs per 1,000 population per day between 2014 and 2018. However, consumption increased by 3% in hospitals over this period.
- There’s a nice section on Candida auris
- ESPAUR reports some good work and outcomes related to training, education, and awareness (e.g. Keep Antibiotics Working and Antibiotic Guardian).
- What a wonderful resource the AMR Fingertips module is: automated data from >90% of NHS laboratories on a range of AMR indicators at our…ahem…fingertips. I am one of the 15k users over the past three years. (As an aside, the volume of traffic is fairly low by popular website standards – but I guess it is somewhat niche!)
ESPAUR is a fantastic resource – it seems that this is the last ESPAUR report related to the UK AMR Strategy from 2013-2018, but I’m confident that ESPAUR will continue to report the successes and challenges of implementing the new five year action plan (from 2019-2024).
Rampant carbapenem-resistant Klebsiella BSIs: a window to a post-antibiotic apocalypse?
People have been talking in apocalyptic terms for years – probably decades – about the threat of AMR. But has this really materialised? MRSA BSIs are now rare in the UK, and C. difficile infections are rarer than they once were. But things are looking considerably gloomier in other parts of the world. For example, a frankly shocking study from a Greek ICU gives us a view of what a post-antibiotic apocalypse may look like…
Who’s going to go for GNBSI? A reflection from HIS 2018

I attended a thought-provoking session at the recent Healthcare Infection Society (HIS) conference in Liverpool on reducing GNBSI (you can download some of the speaker abstracts here). It seems that the hefty majority of E. coli BSIs are rooted in issues outwith the walls of acute hospitals. So the question is, who’s going to tackle these issues to prevent GNBSI? Who’s going to go for GNBSI (sorry, couldn’t resist another pop-culture reference to the ‘80s – who could forget ‘Going for Gold’ with Henry Kelly).
A rapid reflection from Infection Prevention 2017: HCAI ranking according to DALY
I am heading home from an outstanding Infection Prevention 2017. There was a fair bit of discussion about hospital-associated pneumonia (HAP). HAP does not get the attention it deserves and there is more that we can and should be doing to prevent it. Although, we need to keep an eye out for unintended consequences in tackling HAP.
Can we halve Gram-negative BSIs by 50% by 2021? The crowd say “No”

Most of those casting their vote supported Martin’s (somewhat pessimistic) view that we can’t halve Gram-negative BSI by 2021 (see the figure, below). Let me first give you my own, unspoiled opinion (written before the results of this survey were known). I was intending to vote for option 3 (the English can’t, the Dutch might) but I am not even sure of that; actually, I believe that neither the English nor the Dutch can.
