I have posted before about the “postcode lottery” and it’s influence on rates of MRSA, affecting deprived postcodes (or zipcodes!) more than others. But this issue is wider than regional influence. On an international scale, your changes of a bad outcome from infectious disease varies, sometimes wildly, by where you happen to be in the world. A new article in CID on clinical outcomes from carbapenem-resistant Acinetobacter baumannii infections bears this out.
Continue readingmortality
CPE showing its teeth: mortality associated with carbapenem-resistant Gram-negative BSI
Now is a really good time to focus on carbapenem-resistant bacteria. We have spent much of the past 3 years focusing on one particular virus. But now that the clinical issues linked to SARS-CoV-2 are waning for our hospital patients, the threat of carbapenem-resistance in Gram-negative bacteria comes to the fore. An excellent study with far-reaching consequences has been published from Italy. Carbapenem resistance is bad news if you have a BSI: patients with carbapenem-resistant BSI were roughly twice as likely to die as patients with carbepenem-susceptible BSI.
Continue readingCOVID-19 ain’t what it used to be
As the COVID-19 pandemic has swept through various epidemic waves each characterised by a different variant, the trend has been towards more transmissibility but less virulence of SARS-CoV-2. The emergence of the Omicron variant continued this trend, and we are now seeing some data to compare the clinical outcomes of COVID-19 with other variants. A huge Lancet study (1.5m patients!) demonstrates clearly that the risk of hospital attendance, hospitalisation, and death is significantly lower with Omicron compared with Delta. This is important because the consequences of SARS-CoV-2 acquisition are an important factor in deciding on our management strategy – as a hospital group and in general.
Continue readingPreventing healthcare-associated COVID-19
The issue of preventing healthcare-associated COVID-19 is very topical right now, to say the least (see this JAMA commentary), so now is a really good time to review what happened in our hospitals during the ‘first wave’ to help us prevent hospital transmission during the second.
The study was performed during the first wave of COVID-19 in London, between March and mid-April. The focus of the study was on ‘hospital-onset definite healthcare-associated’ (HODHA) COVID-19 infections (with a sample date >14 days from the day of admission). Overall, 58 (7.1%) of 775 symptomatic COVID-19 infections in hospitalised patients were HODHA. Key findings included:
- Compared with community-associated COVID-19, patients with HODHA were more likely to be older, Black Asian or Minority Ethnicity (BAME), have several clinical underlying conditions (e.g. malignancy), and had an increased length of stay after COVID-19 diagnosis. Surprisingly, there was no increased risk of mortality (either 7, 14, or 30-day) or ICU admission.
- There was an interesting analysis of the impact of a delayed positive test (where there was no positive test within 48 hours of symptom development). This occurred in about a third of HODHA cases, and was associated with an increased risk of 30-day mortality.
- A potential source patient (a positive case on the same ward within 14 days of the positive test) was identified for 44/58 HODHA cases.
- There was a correlation between weekly self-reported sickness absence incidence and weekly HODHA incidence.
This is a similar piece of work to our analysis of healthcare-associated COVID-19. The period of time covered was almost identical (from March to mid-April) and the number of HODHAs was very similar (62 in our study compared with 58 in this study). This seems to illustrate how indiscriminate this outbreak has been regionally – a wave of healthcare-associated COVID-19 swept through our hospitals in March/April – and our job now is to reduce the size of this wave over the winter!
ESPAUR 2019: a snazzy facelift
The 2019 edition of the ESPAUR report has recently been published, including data up to and including 2018. The report is an excellent read – here’s a few summary points.
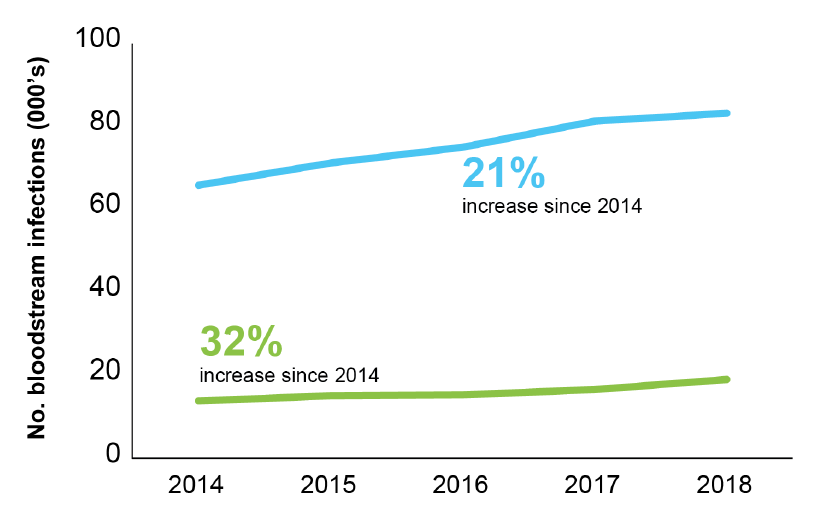
- There’s a series of lovely infographics at the start of the report. I gave myself a challenge: to select the one infographic that told the story of the report. I toyed with the one about a small but increasing number of CPE BSIs (aghhhhh!), and the stark grave-stone themed image of mortality related to carbapenemase-producers, but ended up with this one: alarmingly, the rate of BSI for the seven priority bacterial pathogens rose 22% between 2014 and 2018 to 145 per 100,000 population. (Around half of these were coli). And there’s a certain inexorability about the antimicrobial resistance trends included in this report, with a 32% increase in AMR BSIs comparing 2014 to 2018.
Figure: Trends in BSIs (blue line) and AMR BSIs (green line).
- There were more than 60k antibiotic resistant severe infections in 2018, <150 per day.
- Confirmed CPEs have topped 4k (but this is a gross underestimate of true prevalence). The report makes the case that the rarity of CPE BSIs (142 reported nationally) represents a success of prevention. This is probably true if we compare across the pond and towards the southern reaches of Europe. But difficult to be sure without a control (i.e. what would have happened without the national initiatives etc)? Also, reporting of CPE BSIs to PHE is voluntary and not mandatory, so there will be some degree of under-reporting.
- Related to this, only 50% of diagnostic labs have introduced methods to detect CPE locally. Which links closely with the change in surveillance system for CPEs going forwards – rather than manual voluntary reporting, locally confirmed CPEs will be reported automatically to PHE. However, if only 50% of diagnostic labs have appropriate methods, we’ll still end up under-reporting (but it will be more a more accurate picture than the current process provides).
- 30 day all-cause mortality of invasive CPE infections is 24% (along with the arresting gravestone-themed infographic)! Not sure how helpful it is to make a big point based on unadjusted mortality data…
- Overall consumption of antibiotics continues to decline. Consumption fell from 20 to 18 DDDs per 1,000 population per day between 2014 and 2018. However, consumption increased by 3% in hospitals over this period.
- There’s a nice section on Candida auris
- ESPAUR reports some good work and outcomes related to training, education, and awareness (e.g. Keep Antibiotics Working and Antibiotic Guardian).
- What a wonderful resource the AMR Fingertips module is: automated data from >90% of NHS laboratories on a range of AMR indicators at our…ahem…fingertips. I am one of the 15k users over the past three years. (As an aside, the volume of traffic is fairly low by popular website standards – but I guess it is somewhat niche!)
ESPAUR is a fantastic resource – it seems that this is the last ESPAUR report related to the UK AMR Strategy from 2013-2018, but I’m confident that ESPAUR will continue to report the successes and challenges of implementing the new five year action plan (from 2019-2024).
All BSIs are expensive, not just antimicrobial resistant ones

Eurosurveillance have recently published a study from the TIMER group evaluating the impact of antimicrobial resistance on hospital mortality, excess length of stay (LOS), and cost of BSI in European hospitals. The study highlights the high cost of BSIs, especially when antimicrobial resistant.
