
As you can probably tell from the title, this post comes with a warning: it presents some rather “un-PC” data, but I’ll do my best to deliver it calmly and dispassionately! My old research team from KCL have just published a paper in PLOS Medicine on the association between social and material deprivation, and MRSA.
I’ve been interested in the dynamic between hospital-associated (HA) and community-associated (CA) MRSA for years (not least because it was the subject of my PhD thesis). I wrote a review several years ago on how community MRSA should be seen as a genotypic phenomenon with epidemiological implications. Using this framework, it is possible to get your head around CA strains of MRSA beginning to cause hospital-acquired infections. The aim of this study was to use a large collection of MRSA from across several regions of London to explore the transmission dynamics and epidemiological associations of HA and CA types of MRSA.
The study took around 500 MRSA isolates from hospitals serving a region of London with around 1 million residents. The genotype was defined as HA or CA based on whole genome sequencing data. Then, a series of regression models were constructed to examine associations with demographic, socio-economic data and geographical links. An important factor in the analysis was that the whole dataset was adjusted for the frequency of hospital contact. (As an aside, the proportion of the population with a hospital visit over a 12 month period across the various boroughs in the catchment ranged from 17% to almost 50%; I can only think that this due to pretty terrible access to GPs in some parts of London. Having lived for many years in central London, I have first-hand experience of this – if your GP offers you an appointment in 2 weeks’ time and you have a pressing need to see a doctor, you go to A&E!)
This was a hugely complicated analysis, as illustrated by the almost impossibly intricate co-correlation of variables (see Figure 1 below). Pretty much every variable that was significant in any way was also highly correlated with another variable. This made it very difficult to work out what was actually correlated with MRSA, and what was correlated with something that was correlated with MRSA! After much thought and discussion, we arrived at the grouping of variables that we thought made most sense.
Figure 1: Correlation of variables.

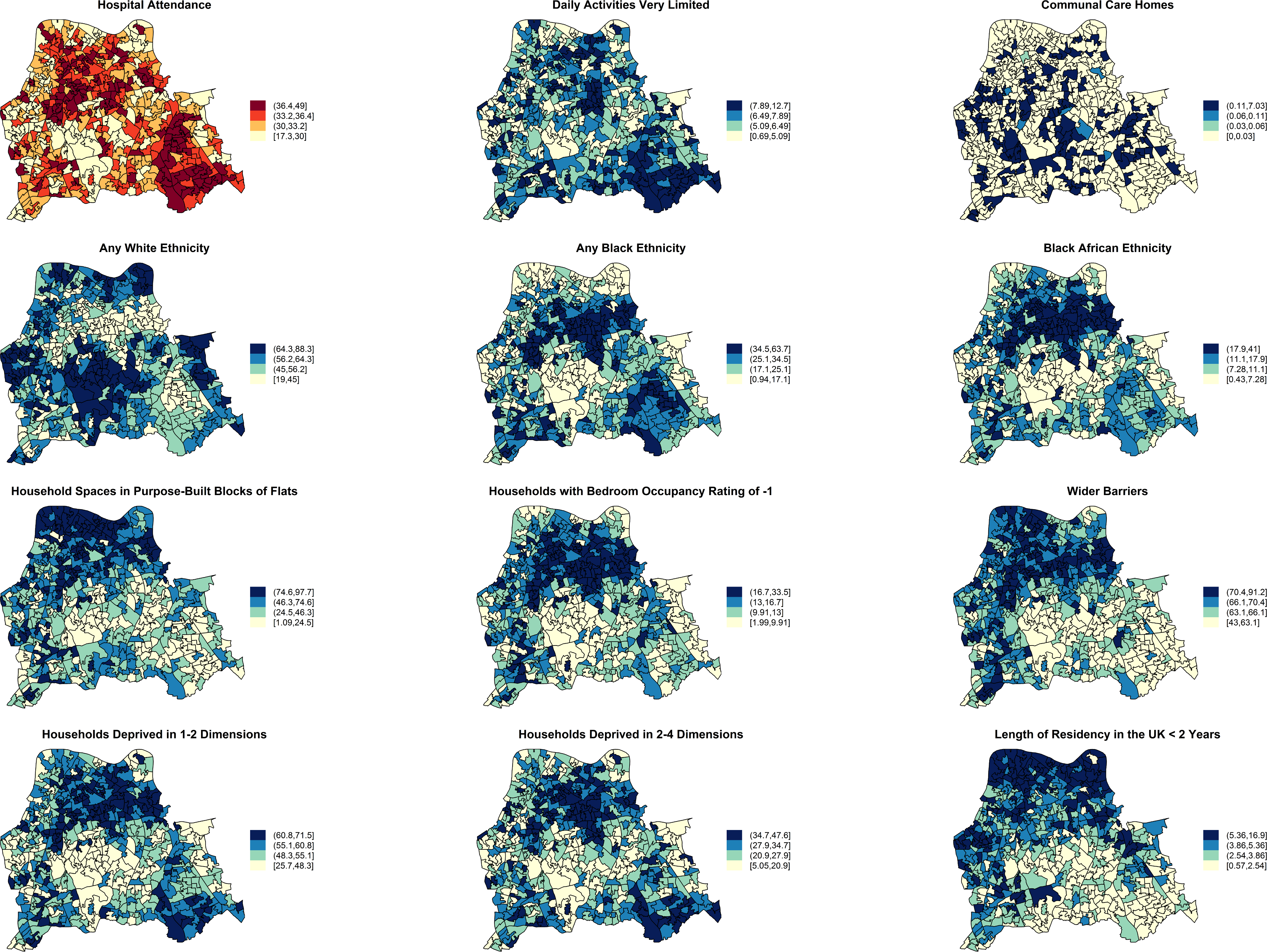
The study tells you some interesting stories about the demographics of London. The fascinating figure below (Figure 2) shows how things get more crowded, more deprived, less British (in the strict sense of which passport is held; I have no point to make about what being British means!), and less white as you move closer to the centre of London (central London is at the top of the area studied). Both CA-and HA-MRSA were associated with household deprivation, which was correlated with hospital attendance. HA-MRSA was also associated with any black ethnic group, poor health, and residence in communal care homes, whereas CA-MRSA was associated with household overcrowding, low income, homelessness, recent immigration to the UK, and black African ethnic group. Being of a white ethnic group was protective against MRSA. This is not the first study to find this profile of risk factors associated with CA-MRSA. In parts of the US where CA-MRSA is now endemic, similar associations with deprivation and ethnic group have been identified. However, I think it’s fair to say this is the most comprehensive evaluation of socio-economic and demongraphic risk factors and MRSA.
Figure 2: Geographical variation in predictors of MRSA.
The other key finding of the study was that there was evidence of spread of CA strains in the community but not HA strains. Areas adjacent to deprived areas where CA-MRSA was more common were themselves at greater risk of CA-MRSA, indicating community transmission of CA-MRSA. This suggests that little or no transmission of HA-MRSA strains occurs in community settings.
So, what is underpinning these co-correlated associations between CA strains of MRSA and material / social deprivation? Is this to do with hygiene? Education? Diet? Ethnic group? All of the above? It’s very difficult to be certain. But it is clear from this and other studies that community MRSA preys on the poor and deprived.
I wonder, does anybody fancy participating in a cluster randomised community-based intervention study to get to the bottom of what is driving these associations? One arm could be a hygiene intervention and one arm could be an educational intervention. I can’t think of a discrete intervention that would address poverty and overcrowding, but any suggestions welcome!
Cover image credit: Geograph.org.uk.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
