I am heading home from an outstanding Infection Prevention 2017. There was a fair bit of discussion about hospital-associated pneumonia (HAP). HAP does not get the attention it deserves and there is more that we can and should be doing to prevent it. Although, we need to keep an eye out for unintended consequences in tackling HAP.
An excellent paper published in PLOS Medicine at the back-end of 2016 estimated the burden of six HCAI on European population health using disability-adjusted life-year (DALY) incidence modelling. The DALY is a composite health measure estimating years lived with disabilities (YLDs) following the onset of a disease and of life years lost due to premature mortality (YLLs) compared with standardized life expectancy. The aim of the study was to produce an adjusted HCAI prevention priority list. The study used data from the 2011-12 ECDC PPS, finding that the ranking of the six HCAIs varied considerably when ranked by number of cases vs. DALY adjusted burden (Figure 1 and 2).
Figure 1: HCAIs according to their number of cases per year (x-axis), number of deaths per year (y-axis), and DALYs per year (width of bubble).
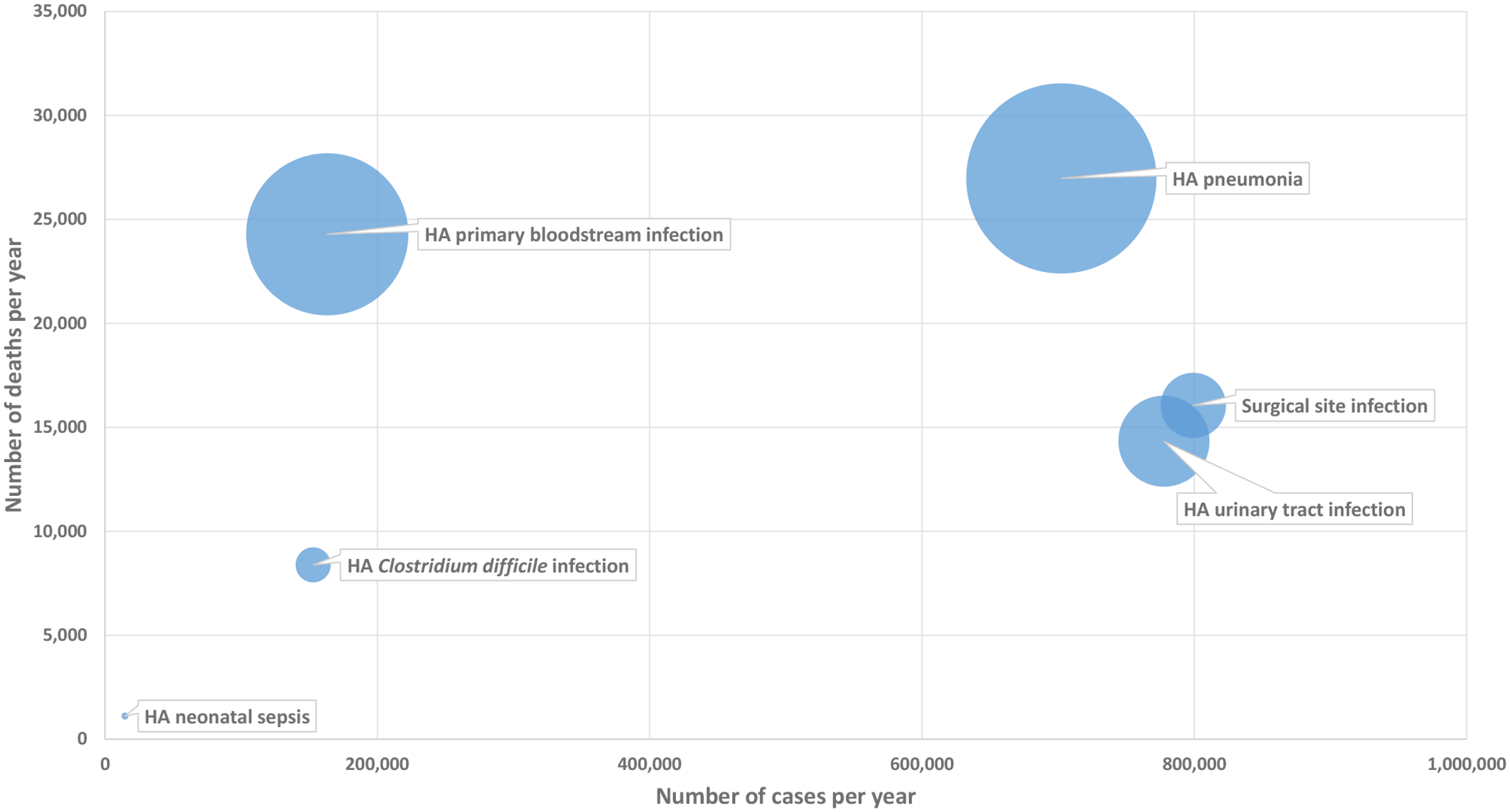
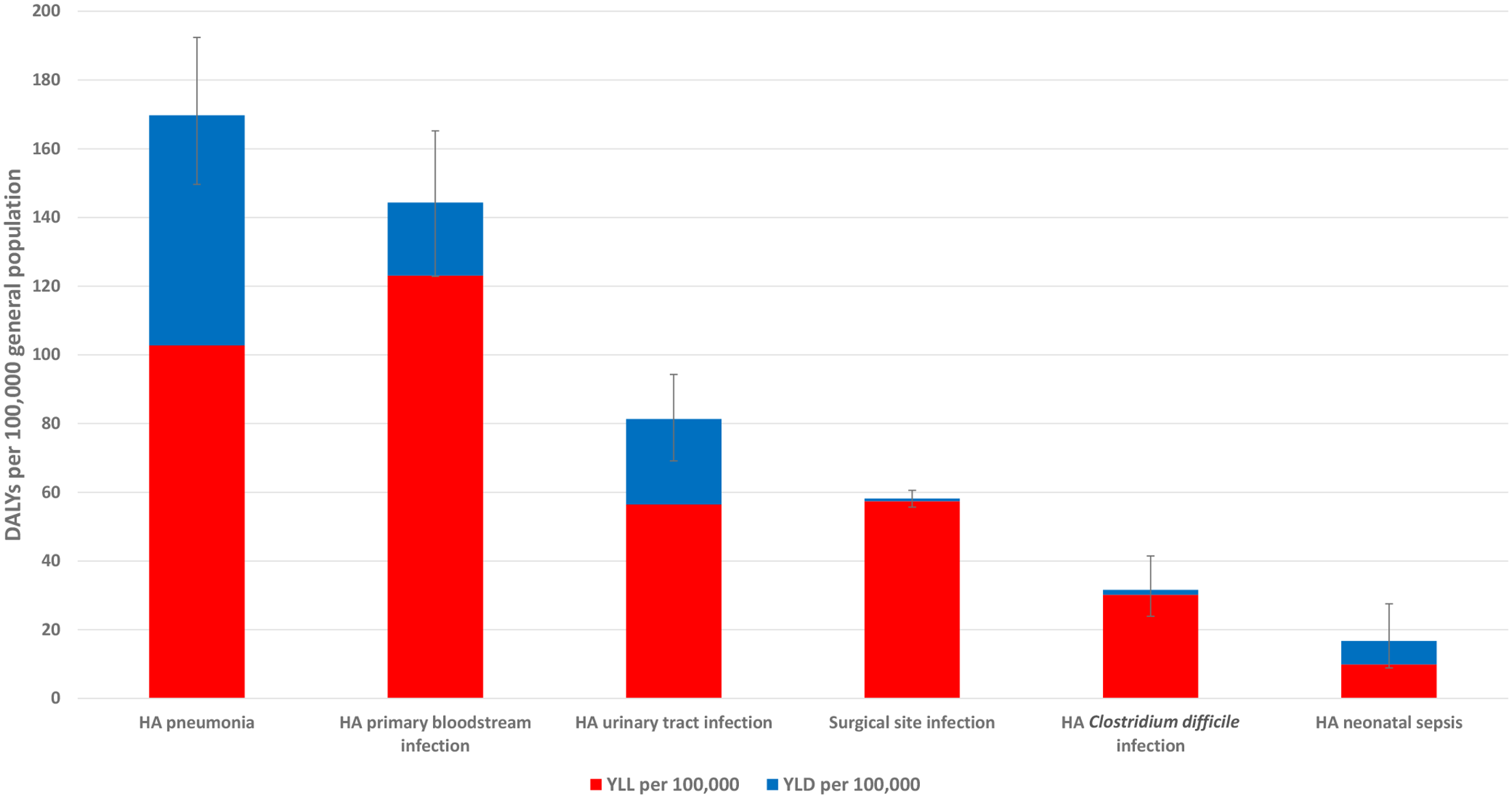
Figure 2: Estimated annual burden of six healthcare-associated infections in DALYs per 100,000 population (median and 95% uncertainty interval), split between YLLs and YLDs.
Now, if I were to rank these six HCAIs in order of priority currently given to them by most IPC programmes, it would look something like the bottom row of Figure 3. As you can see, the focus of most IPC programmes does not match this priority list!
Figure 3: Ranking of HCAI. Top row = by number of cases. Middle row = by DALY-adusted burden. Bottom row = a ‘real world’ ranking based on prioritisation by IPC programmes. I should add, in stark contrast to the careful and scientific QALY-adjusted burden ranked list of HCAIs, my ‘real world’ ranking has come purely from my own head, based on my perception of focus and resource allocation.

The clear message from this study is that we would make most impact on the burden of HCAI if HAP was our number one priority, which it currently most certainly is not. A HAP prevention bundle (including a focus on oral care and mobility) would not be complex to put together or implement (in theory) but, according to a recent review, none exist!
And finally to a slightly controversial idea raised by fellow-blogger Martin Kiernan at IPS. Pneumonia is ‘affectionately’ known as “The old man’s friend”, because it is commonly the terminal event in older people. If we do effectively prevent HAP in this group, then it is highly likely that another common cause will emerge as the terminal event in this group. So, perhaps quality-adjusted life years (QALYs) need to feature in this discussion?
I would be interested in any feedback on my ranking of HCAIs, and some intel on any HAP prevention bundles that are currently available.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

I was highly surprised by the outcome of that PLoS Med study as HAP is something so non-definable. In intubated patients (HAP is then called VAP) you can perform bronchoscopy to distinguish colonization from infection (although the approach is hardly used). In my experience there is no objective definition for HAP and we just count what physicians want to treat (any patient with some fever, sputum production and a chest X-ray on which a “possible starting infiltrate” cannot be ruled out). And Martin can be reassured: For the better definable infection, VAP, recent data clearly show that its attributable mortality is low (at least much lower than always assumed) and the clinical presentation of HAP usually doesn’t resemble the disease caused by the “old man’s friend” pneumococcus. Bottomline (for me) before we throw out bundles on HAP let’s find workable and reasonably objective diagnostic criteria for HAP. No need for VAP. Just use SDD.
LikeLike
Thanks Marc useful comment. We know from local experience that “HAP” is hopelessly over-diagnosed, so I wonder how a DALY analysis adjusted for the risk of over-diagnosis would look?!
LikeLike
The outcome of the study are surprising and deserve to be taken into consideration by IPC programmes.
LikeLike