A fantastic new study from Brett Mitchell’s prolific group in Australia has recently been published in Lancet Infectious Diseases and the results are pretty spectacular. A fairly low cost intervention of an extra 3 hours of cleaning and disinfecting shared medical equipment each day resulted in a whopping 35% reduction in HCAI in a randomised controlled trial. I’m delighted to say that Prof Brett Mitchell will be introducing an IPC Journal Club on this study next Wednesday (register here).
Continue readingintervention study
How can we stop nursing homes nurturing MRSA?

There is an emerging feeling that we need to start spreading the focus of infection prevention and control beyond acute hospitals. There has always been a sense that standards of infection control outside of acute settings are, shall we say, “different” to acute hospitals (aka non-existent) so it’s great to see a study of an infection control intervention in nursing homes.
The study was a cluster randomised controlled trial of MRSA screening, decolonisation and enhanced environmental disinfection vs. standard precautions in 104 of 157 nursing homes in a Swiss region. The authors chose a rather unusual, pragmatic endpoint of the prevalence of MRSA colonisation after 12 months.
European approaches to MDR-GNR prevention and control

I was privileged to be asked to speak at the inaugural Healthcare Infection Society Middle East Summit in Dubai this week on ‘European approaches to MDR-GNR prevention and control’. You can download my slides here.
I began with a (probably too lengthy) preamble outlining some overall points:
- CRE is a big deal in Europe, especially in the UK, and has prompted unprecedented action on a national level in the form of a Toolkit, a Patient Safety Alert and a letter to all CEOs requesting (demanding?) an action plan. The political picture is similar elsewhere in Europe and in the USA. Although this level of government scrutiny can be challenging, on the whole I think it’s beneficial, and is probably a sizeable factor in the successes achieved with MRSA and CDI.
- Do we go universal or targeted? There’s been much discussion recently about abandoning traditional targeted (aka vertical) approaches in favour of universal (aka horizontal). Interesting, all guidelines that I could lay my hands on favoured a targeted approach for MDR-GNR, centred around screening and isolation of carriers.
- Where is the evidence? We are hamstrung by the lack of high quality studies telling us with any certainty what works to control MDR-GNR. Pretty much all studies to date are either performed in an outbreak setting (regression to the mean…) or include multiple interventions (which worked?), or both. The few studies that evaluated a single intervention in an endemic setting are underpowered to deliver a meaningful conclusion. So, we need bigger and better studies!
- How do you produce good guidelines – who is on the guideline writing dream team, and what are the key pitfalls to avoid. Plus, importantly, how to good guidelines translate through a good policy into good practice?
What works to control antibiotic-resistant bacteria in the ICU? A two-for-the-price-of-one study
Not content with a single well-planned study to provide information on what works to control multidrug-resistant organisms (MDROs) in the ICU, the MOSAR study group published an interrupted time series and a cluster randomized trial of various interventions in the Lancet ID. This makes the study rather complex to read and follow, but there are a number of important findings.
Interrupted time series – ‘hygiene’ intervention (chlorhexidine and hand hygiene)
Following a 6-month pre-intervention period, a 6-month interrupted time series of a ‘hygiene’ intervention (universal chlorhexidine bathing combined with hand-hygiene improvement) was performed. The key outcomes were twofold: whether there was a change in trend during each phase, and whether there was a step-change between the phases. The hygiene intervention effected a trend change reduction in all MDROs combined and MRSA individually, but not in VRE or ESBLs (Table). However, there was no step-change compared with the baseline period.
Table: Summary of reduced acquisition of all MDROs combined, or MRSA, VRE and ESBLs individually.

Cluster RCT – screening and isolation
In the 12-month cluster RCT of screening and isolation, the 13 ICUs in 8 European countries were randomized to either rapid screening (PCR for MRSA and VRE plus chromogenic media for ESBL-Enterobacteriaceae) or conventional screening (chromogenic media for MRSA and VRE only). When analysed together, the introduction of rapid or conventional screening was not associated with a trend or step-change reduction in the acquisition of MDROs (Table). In fact, there was an increase in the trend of MRSA acquisition. When comparing rapid with conventional screening, rapid screening was associated with a step-change increase in all MDROs and ESBLs.
Discussion
- The study suggests, prima facie, not to bother with screening and isolation. Indeed, the authors conclude: “In the context of a sustained high level of compliance to hand hygiene and chlorhexidine bathing, screening and isolation of carriers do not reduce acquisition rates of multidrug-resistant bacteria, whether or not screening is done with rapid testing or conventional testing”. However, the major limitation here is that many of the ICUs were already doing screening and isolation during the baseline and hygiene intervention phases! I checked the manuscript carefully (including the supplemental material) to determine exactly how many units were, but it is not disclosed. To make this conclusion, surely the cluster RCT should have been ‘no screening and isolation’ vs. ‘screening and isolation’.
- The increasing trend of MRSA associated with screening and isolation by either method, and step-change increases in all MDROs and ESBLs associated with rapid screening are difficult to interpret. Is an increase in acquisition due to screening and isolation plausible? Can more rapid detection of carriers really increase transmission (the turnaround time was 24 hours for rapid screening, and 48 hours for chromogenic screening)? The rapid screening arm also included chromogenic screening for ESBLs, whereas the conventional screening arm did not, so perhaps this apparent increase in acquisition is due to improved case ascertainment somehow?
- Looking at the supplemental material, a single hospital seemed to contribute the majority of MRSA, with an increasing trend in the baseline period, and a sharp decrease during the hygiene intervention. There’s a suspicion, therefore, that an outbreak in a single ICU influenced the whole study in terms of MRSA. Similarly, a single hospital had a sharp increase in the ESBL rate throughout the screening intervention period, which may explain, to a degree, the increasing trend of ESBL in the rapid screening arm.
- There was an evaluation of length of stay throughout the study phases, with a significant decrease during the hygiene intervention (26%), a significant increase during the rapid screening intervention, and no significant change during the conventional screening intervention. It seems likely that improved sensitivity of rapid screening identified more colonized patients who are more difficult to step down, resulting in an overall increase in length of stay.
- The carriage of qacA and qacB was compared in the baseline and hygiene intervention phase, finding no difference in carriage rate (around 10% for both). This does not match our experience in London, where carriage rates of qacA increased when we introduced universal chlorhexidine bathing. However, this was restricted to a single clone; the acquisition of genes associated with reduced susceptibility to chlorhexidine seems to be clone-specific.
- ICUs varied from open plan to 100% single rooms. Whilst the average proportion of patients in single rooms (15-22%) exceeded the average requirement of patients requiring isolation (around 10%), there was no measure of unit-level variation of single room usage. Since the study was analysed by cluster, the lack of single rooms on some units could have been more important than would appear from looking at the overall average. Put another way, a 100% open plan unit would have been forced to isolate all carriers on the open bay, and vice versa for a 100% single room unit.
- The impact of the various interventions was moderate, even though a ‘high’ MRDO rate was necessary for enrollment (MRSA bacteraemia rate >10%, VRE bacteraemia rate >5%, or ESBL bacteraemia rate >10%). Would the impact of screening and isolation be different on a unit with a lower rate of MDROs? It’s difficult to tell.
- Some of the microbiology is quite interesting: 8% of MRSA were not MRSA and 49% of VRE were not VRE! Also, 29% of the ESBLs were resistant to carbapenems (although it’s not clear how many of these were carbapenemase producers).
In summary, this is an excellent and ambitious study. The lack of impact on ESBL transmission in particular is disappointing, and may lead towards more frequent endogenous transmission for this group. The results do indicate screening and isolation did little to control MDRO transmission in units with improved hand hygiene combined with universal chlorhexidine. However, we need a ‘no screening and isolation’ vs. ‘screening and isolation’ cluster RCT before we ditch screening and isolation.
Can the introduction of 6 copper items into ICU rooms really reduce the rate of HAI by >50%?
The recent article by Salgado et al.in the ICHE special edition is the long-awaited copper study: a multi-centre evaluation of the clinical impact of introducing 6 copper alloy high-touch sites into the rooms of patients on three ICUs. I’ve been looking forward to getting my hands on this study for some time!

Patients (n=614 following exclusions) were randomized to intervention ‘copper’ rooms and control ‘non-copper’ rooms in three USA ICUs over an 11 month period. The only difference between the rooms was the presence of six items made of copper alloy, comprising bedrails, overbed tables, IV poles and visitor chair arms in all rooms and the nurse call button, computer mouse, computer palm rest and rim of a touch-screen monitor in other rooms.
Patients admitted to copper rooms were significantly less likely to acquire healthcare-associated infection (HAI) or colonization with MRSA / VRE (Figure).
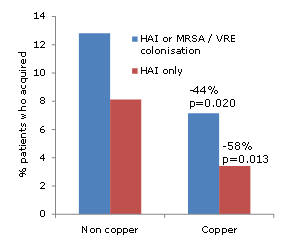
Figure: difference in acquisition rate between patients admitted to ‘copper’ or ‘non-copper’ rooms
The authors also make an interesting association between the degree of contamination in patient rooms and the risk of acquisition. However, since sampling was performed weekly regardless of a patient’s infection or colonization status, it is not possible to determine whether this association is causal or simply due to the fact that infected / colonized patients are likely to shed more bacteria into the hospital environment.
The study team should be commended for the careful design and attention to detail in the execution of the study. For example, they performed a daily census of the items in the study to determine exactly who was exposed to copper surfaces, and for how long. This indicated that only half of the patients in ‘copper’ rooms were exposed to all six copper items for the duration of their stay, and 13% of patients in the ‘non-copper’ arm were exposed to some copper items during their stay. It’s important to note that the analysis was performed on an ‘intention to treat’ population, i.e. all patients randomized to the two groups, regardless of which items they were actually exposed to. It would have been interesting to see a sub-analysis on the ‘per protocol’ population (i.e. those patients admitted to ‘copper’ rooms and exposed to all six copper items vs. those patients admitted to ‘non-copper’ rooms and exposed to no copper items). Also, I’m not sure why they chose to analysis % acquisition rather than a comparison of rates between the groups. And then there’s the salary support and grant funding to some authors (not directly related to this study) from the Copper Development Association. Notwithstanding these limitations, it does seem that the introduction of copper high-touch surfaces does reduce the transmission of hospital pathogens.
The scale of the difference is incredible. And I mean just that. It lacks credibility. Many will dismiss the study simply because of the scale of the difference between the groups. So, can the introduction of 6 copper items into ICU rooms really reduce the rate of HAI by >50%?
The degree to which contaminated surfaces contribute to the transmission of pathogens is up for debate. I was asked to give a talk at APIC 2012 on the role of the environment. Prior to the talk, I asked the expert faculty a question: ‘What is your estimation of the % of allC. difficile transmission in hospitals that is mediated, directly or indirectly, by contamination of the inanimate environment?’ The answers ranged from 25-75%, reflecting the uncertainty on this issue.
A recently published study by Johns Hopkins provides some illuminating findings (albeit indirectly). Extrapolating unadjusted acquisition rates from all study cohorts indicates that if rooms had been disinfected using hydrogen peroxide vapour (HPV) after every discharge, the overall rate of acquisition of MDROs would have been halved. Whilst it’s not feasible to disinfect all rooms using HPV at patient discharge, this does add some weight to the scale of the reduction identified in this copper study.
It seems that the introduction of a handful of copper alloy high-touch sites had a profound impact on HAI rates. On reflection, I do believe it possible that the scale of reduction in study is “real”. However, questions remain over the practicality and durability of the widespread adoption of copper alloy surfaces in healthcare.
Article citation:
More single rooms = less acquisition. A simple equation?
This isn’t exactly hot off the press (published in 2011) but I’ve only just come across it; it’s a great article and worth revisiting. Many hospitals worldwide suffer a chronic lack of single rooms to place patients requiring contact precautions, but also for patients with other needs such as increased privacy and dignity. There are pros and cons associated with increasing the proportion of single rooms, with a high proportion of single rooms usually requiring a higher staff:patient ratio, and patients in single rooms often having less staff contact and more likely to suffer feelings of isolation. The evidence that an increase in the proportion of single rooms reduces the transmission of healthcare-associated infection has been somewhat equivocal.
This Canadian study evaluated the impact of ‘privatization’ of an ICU. In March 2002, a 24-bed ICU (comprising two 10-bed rooms and four single rooms) was moved to a new 100% single room unit. A 25-bed ICU in a sister hospital (comprising 2, 5, 6 or 8-bed rooms) did not undergo any change in configuration and served as a comparison unit. Importantly, the two units shared the same infection control team, policies and practices. Patients admitted between 2000 and 2005 were studied for the acquisition of a range of pathogens. A unique and useful aspect of the study was to divide microbes into likely endogeneous or exogeneous acquisition. The key result reported was the change in rate ratio of the intervention ICU compared with the comparison ICU before and after the date of privatization of the intervention ICU. This was effectively an estimate of the percentage reduction in the rate in the intervention hospital associated with privatization.
Significant reductions where shown in most pathogens associated with exogenous acquisition, including C. difficile (43%), MRSA (47%) and Acinetobacter spp. (53%), and a substantial but non-significant reduction in Stenotrophomonas maltophilia (52%) (Figure). In addition, a combined analysis of C. difficile, MRSA and VRE also showed a significant reduction of 54%. Significant reductions were also shown for some pathogens in the exogenous/endogenous acquisition group, including Klebsiella spp. (38%). There was no significant change (4%) in the rate of coagulase-negative staphylococci and most other pathogens associated with endogenous acquisition. Perhaps not surprisingly, the authors also reported a reduction in the overall length of stay associated with the intervention.

Figure: Change in the acquisition rate ratio of the intervention vs. comparison ICU before and after before (2001-2002) vs. after (2003-2005) privatisation. (* Not statistically significant.)
As with all studies, this one is not without criticism. However, there are several aspects that I find particularly convincing. Firstly, whilst there were differences in the configuration of the two ICUs, the inclusion of a comparison unit was an important strength. Secondly, the authors evaluated all available pathogens, rather than focusing on an individual MDRO. Thirdly, and perhaps most convincingly, most pathogens associated with exogeneous infections were affected by the intervention whereas most pathogens associated with endogenous acquisition were not. Additional strengths include several “data-check” sensitivity analyses and an additional model to provide evidence that these were not transient reductions associated with moving to a new, clean unit. Many if not all of these important strengths are lacking from similar studies that have returned a negative result.
The simple equation that more single rooms = less acquisition of pathogens is firmly supported by this study. However, infection rates are not the only factors to be considered when contemplating a move to 100% single rooms. Staffing levels, patients views and up-front costs must be factored into the decision to move towards 100% single rooms.
Article citation:
Improved terminal disinfection using hydrogen peroxide vapour (HPV) or bleach to control C. diff
A prospective before-after study at the 900 bed St. John’s Mercy Medical Center evaluated the impact of an HPV intervention focused on the terminal disinfection of rooms used by patients with multidrug-resistant organisms and C. difficile. HPV was introduced on a priority scale accounting for the target pathogen and the risk associated with the unit. Due to local prevalence, most of the rooms decontaminated using HPV were vacated by patients with C. difficile infection (CDI). Hence, the authors evaluated the impact of introducing HPV on the rates of CDI.
The rate of CDI was static prior to the introduction of HPV, with no significant change in rate from 2007 to 2008 (Figure). Hence, this study was performed in a truly endemic setting in contrast to a previous study of a similar design by Boyce et al., which was performed in a “hyper-endemic” setting. When HPV was introduced in 2009 (along with enhanced conventional methods comprising quadruple bleach disinfection for rooms that could not be disinfected using HPV), the rate of CDI fell by 37% from 0.9 to 0.5 cases per 1000 patient days (p<0.0001) (see chart below).
Chart showing the rate of C. difficile infection before and after the implementation of HPV or quadruple bleach disinfection for the terminal decontamination of patient rooms.

Recent data have shown that patients admitted to rooms previously occupied by a patient with C. difficile are at an increased risk of developing C. difficile infection. Thus, it seems logical that improving the efficacy of terminal disinfection would result in reduced rates of CDI. Furthermore, the scale of reduction in CDI incidence was remarkably similar to the study by Boyce et al. (37% vs. 39%), though in this previous study, the 39% hospital wide reduction was not statistically significant.
The major criticism of the study is that HPV and quadruple bleach disinfection were implemented more or less simultaneously so it’s not possible to attribute the reduction to HPV alone. This is complicated by the fact that quadruple bleach disinfection was implemented for all C. difficile rooms in mid-2008, 6 months prior to the introduction of HPV. So, it is possible in theory to do a sub-analysis of corresponding months during the period when quadruple bleach disinfection alone compared with HPV plus quadruple bleach disinfection was in operation. However, this sub-analysis was not performed. A previous study by the same group showed that quadruple bleach disinfection was necessary to eliminate A. baumannii and MRSA from surfaces, and that HPV was microbiologically superior to quadruple bleach disinfection. Thus, since HPV has time and efficiency savings compared with quadruple bleach disinfection, it is cost effective to use HPV in this setting.
The authors undertook a careful evaluation of hand hygiene and glove / gowning compliance, showing that these were not significantly different comparing the pre-intervention and intervention periods. They also evaluated the use of key antimicrobial agents and found that there were small but statistically significant changes in antimicrobial usage, which may have confounded the association with improved disinfection. However, levofloxacin use (one of the high risk CDI drugs) increased significantly in 2009 and there was still a significant reduction in CDI.
The paper includes some useful data on feasibility and safely aspects of implementing HPV, and the ‘priority scale’ (Appendix) for deciding which rooms were disinfected using HPV is rational and will help other hospitals decide on a similar priority scale.
Several other points of interest are reported. For example, the significant reduction in CDI was achieved whilst adhering to US C. difficile control guidelines, which recommend the use of gloves and alcohol based hand products (rather than hand washing with soap and water) for treating patients with CDI in endemic settings. They also held patients who had CDI in contact precautions for the duration of their stay, not just until symptoms resolved.
This study shows that more effective removal of C. difficile spores from the rooms of patients when they are discharged through enhanced conventional methods combined with the implementation of HPV reduces the hospital-wide incidence of CDI. The authors conclude: ‘implementation of an enhanced hospital-wide terminal cleaning program revolving around HPV decontamination of targeted hospital rooms was practical, safe, and associated with a significant reduction in the endemic rate of CDI at our hospital.’
Article citation: Manian FA, Griesnauer S, Bryant A. Implementation of hospital-wide enhanced terminal cleaning of targeted patient rooms and its impact on endemic Clostridium difficile infection rates. Am J Infect Control in press.
Mitigating the increased risk from the prior room occupant through HPV room disinfection
The role of surface contamination is increasingly recognised in the transmission of certain nosocomial pathogens1. The most compelling evidence comes from the finding that admission to a room previously occupied by a patient infected or colonised with some multidrug-resistant organisms (MDROs) increases the risk of acquiring that MDRO for the subsequent room occupant by a factor of two or more1-3. Conventional cleaning and disinfection does not reliably remove all environmental MDROs4,5. Hence, it seems that inadequate terminal disinfection of hospital rooms explains the association with the increased risk of acquisition from the prior room occupant. It follows, then, that improvements in terminal disinfection should reduce the levels of residual contamination and the transmission of pathogens through this route. A recent study from Johns Hopkins Hospital tested this hypothesis through the introduction of hydrogen peroxide vapour (HPV) terminal disinfection of selected patient rooms6.
A 30-month prospective cohort intervention study was performed on 6 high-risk units (5 ICUs). HPV was implemented on 3 of the units following a 12-month pre-intervention phase. Clinical impact was assessed by a cohort study. Each patient admitted to any study unit during both phases was included in one of three cohorts:
- ‘MDRO-standard’ Patients admitted to a room where the prior room occupant had an MDRO and the room was disinfected using standard methods.
- ‘MDRO-HPV’Patients admitted to a room where the prior room occupant had an MDRO and the room was decontaminated using HPV
- ‘No MDRO-standard’ Patients admitted to a room where the prior room occupant was not known to have an MDRO and the room was disinfected using standard methods.
The key finding was that patients admitted to rooms decontaminated using HPV were 64% less likely to acquire any MDRO (incidence rate ratio [IRR] of the MDRO-HPV vs. MDRO-standard cohorts = 0.36, confidence interval CI=0.19-0.70, p<0.001) (see chart below).
Chart showing the MRDO acquisition rate in the three patient cohorts.

‘MDRO-standard’ = Patients admitted to a room where the prior room occupant had an MDRO and the room was disinfected using standard methods. ‘MDRO-HPV’ = Patients admitted to a room where the prior room occupant had an MDRO and the room was decontaminated using HPV.
‘No MDRO-standard’ = Patients admitted to a room where the prior room occupant was not known to have an MDRO and the room was disinfected using standard methods.
The difference between cohorts was adjusted for patient level variables such as length of stay, morbidities and other variables that could explain the difference. This means that the difference between cohorts is attributable to HPV alone. When broken down into individual MDROs, the largest reduction was shown for VRE (a 75% reduction, p<0.0001). HPV provided a protective effect for the other MDROs assessed (C. difficile, MRSA and MDR-Gram-negative rods), but differences for these individual pathogens were not statistically significant.
Surprisingly, even when the prior room occupant was not known to have an MDRO, HPV reduced the risk of acquisition by 51% (comparing the MDRO-HPV with the No MDRO-standard cohort). You’d expect the acquisition rate in the ‘MDRO-HPV’ cohort to match the ‘No MDRO-standard cohort’. In fact, it is lower. This is likely due to survival of contamination from previous occupants, unrecognised colonisation or introduction by healthcare workers.
Environmental impact was assessed by sampling each patient room on all units monthly for the last 3 months of the pre-intervention phase and the first 6 months of the intervention phase. Swabs were collected from all patient rooms, occupied or unoccupied, regardless of patient status. The overall percentage of rooms contaminated with one or more MDRO was reduced significantly when HPV was in operation. Further, rooms contaminated with multiple MDROs, occasions when the MDRO from room differed from the room occupant’s known MDRO and MDROs cultured from empty rooms were less likely when HPV was in operation.These changes are due to improved terminal disinfection using HPV.
Whilst this study is one of the few to evaluate patient outcomes in addition to environmental impact of a no-touch automated room disinfection system7. it does have several limitations, some of which are highlight in an accompanying editorial8. Firstly, the rooms or units were not randomized to an intervention arm, which could have introduced bias. Secondly, whilst the conventional disinfection methods were optimized prior to the introduction of HPV, more could have been done to improve the efficacy of conventional methods which may have over-estimated the impact of HPV. Thirdly, the low prevalence of acquisition (especially for MDROs besides VRE) made detecting changes in incidence difficult. Fourthly, whilst the infection rates in the three cohorts did not change significantly with study phase and the clinical impact on an individual patient level was impressive, overall unit level changes in rates of infection were not reported.
The study has important implications for the proportion of transmission that is likely to involve contaminated surfaces. Extrapolating unadjusted data from the study indicates that 16.7% of the acquisitions that occurred during the study were attributable directly to the prior room occupant. This figure most likely underestimates the total contribution of contaminated surface to nosocomial transmission because contaminated surfaces are likely to be involved indirectly in transmission during the stay of affected patients1.
In summary, HPV disinfection significantly reduced the risk of patients acquiring MDROs from previous room occupants in high-risk settings. Furthermore, HPV also provides a protective effect even when the prior room occupant was not known to be infected or colonised with an MDRO. These clinical findings are supported by environmental data showing that HPV disinfection improves the efficacy of terminal disinfection, thus reducing environmental contamination. Whilst the study is not without its limitations, it takes the question of how to tackle hospital environmental contamination forward a pace or two.
Article citation: Passaretti CL, Otter JA, Reich NG et al. An evaluation of environmental decontamination with hydrogen peroxide vapor for reducing the risk of patient acquisition of multidrug-resistant organisms. Clin Infect Dis 2013; 56: 27-35.
References:
1. Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect Control Hosp Epidemiol 2011; 32: 687-699.
2. Drees M, Snydman D, Schmid Cet al. Prior environmental contamination increases the risk of acquisition of vancomycin-resistant enterococci. Clin Infect Dis 2008; 46: 678-685.
3. Huang SS, Datta R, Platt R. Risk of acquiring antibiotic-resistant bacteria from prior room occupants.Arch Intern Med 2006; 166: 1945-1951.
4. Manian FA, Griesenauer S, Senkel Det al. Isolation of Acinetobacter baumannii complex and methicillin-resistant Staphylococcus aureus from hospital rooms following terminal cleaning and disinfection: can we do better? Infect Control Hosp Epidemiol 2011; 32: 667-672.
5. French GL, Otter JA, Shannon KP, Adams NM, Watling D, Parks MJ. Tackling contamination of the hospital environment by methicillin-resistant Staphylococcus aureus (MRSA): a comparison between conventional terminal cleaning and hydrogen peroxide vapour decontamination. J Hosp Infect 2004; 57: 31-37.
6. Passaretti CL, Otter JA, Reich NGet al. An evaluation of environmental decontamination with hydrogen peroxide vapor for reducing the risk of patient acquisition of multidrug-resistant organisms. Clin Infect Dis2013; 56: 27-35.
7. Otter JA, Yezli S, Perl TM, Barbut F, French GL. Is there a role for “no-touch” automated room disinfection systems in infection prevention and control? Submitted. J Hosp Infect 2013; 83: 1-13.
8. McDonald LC, Arduino M. Climbing the evidentiary hierarchy for environmental infection control. Clin Infect Dis 2013; 56: 36-9.
