A helpful new review and meta-analysis asks whether treating hard surfaces or linen reduces healthcare-associated infections. The review identified only a small number of studies that had both a copper-related intervention related to surfaces and/or linen and an outcome related to HCAI. But the meta-analysis of the seven studies found that, overall, the risk of HCAI was reduced by 27% (risk ratio 0.73, 95% confidence interval 0.57–0.94).
Continue readingcopper
An overview of the options for antimicrobial surfaces in hospitals

I’ve been asked to write a chapter providing an overview of options for antimicrobial surfaces in hospitals for a Springer book. As a result of the preliminary literature reviews for this chapter, I’ve summarized the various available options for antimicrobial surfaces in hospitals in this post.
A number of different interventions aimed at improving environmental hygiene have been evaluated. Switching from one disinfectant to a product with superior microbiological efficacy in particular has been shown to reduce transmission.1-6 However, one of the problems with available disinfectants is the lack of residual effect, meaning that recontamination occurs quickly.7,8 An attractive option is to somehow make surfaces antimicrobial to exert a continuous reduction in the level of contamination. A recent review by Prof Hilary Humphreys provides a useful overview of the various approaches to antimicrobial surfaces.9 There are several approaches to making a hospital surface ‘antimicrobial’:
- Permanently ‘manufacture in’ an agent with antimicrobial activity (e.g. copper or a chemical).
- Periodically apply an agent with antimicrobial activity (e.g. copper containing liquid agents, or chemical disinfectants with residual activity).
- Physically alter the properties of a surfaces to make it less able to support microbial contamination or easier to clean (e.g. antibiofilm surfaces).
The table below provides an overview of the various options available to make a hospital surface antimicrobial.
| Candidate | Application | Pros | Cons |
| Metals | |||
| Copper | Manufactured in / liquid disinfectant | Rapidly microbicidal; large evidence-base; evidence of reduced acquisition. | Sporicidal activity equivocal; cost, acceptability and durability may be questionable. |
| Silver | Manufactured in / liquid disinfectant | Broadly microbicidal. | ? sporicidal; tolerance development; relies on leaching so surface loses efficacy over time. |
| Chemicals | |||
| Organosilane | Liquid disinfectant | Easy to apply. | Limited microbicidal activity; questionable “real-world” efficacy. |
| Light-activated (e.g. titanium dioxide or photosensitisers) | Manufactured in / liquid disinfectant | Broadly microbicidal; can be activated by natural light. | ? sporicidal; requires light source for photoactivation (some require UV light); may lose activity over time. |
| Quaternary ammonium compound based | Liquid disinfectant | Easy to apply. | Limited microbicidal activity; largely untested real-world activity. |
| Triclosan | Manufactured-in / liquid disinfectant | Already adopted in some consumer markets. | Resistance / tolerance development; relies on leaching so surface loses efficacy over time. |
| Polycationic e.g. polyhexamethylene biguanide, PHMB | Liquid disinfectant | Easy to apply. | Limited microbicidal activity; questionable “real-world” efficacy. |
| Physical alteration of surface properties | |||
| “Liquid glass” (silicon dioxide) | Liquid application | Reduces deposition; improves ‘cleanability’. | Not microbicidal; some evidence of reduced contamination; unknown required frequency of application. |
| Sharklet pattern | Manufactured-in | Reduces deposition; reduced. biofilms. | Not microbicidal; not feasible to retrofit. |
| Advanced polymer coatings (e.g. polyethylene glycol PEG, superhydrophobic/philic, zwitterionic) | Manufactured-in | Reduces deposition; some can be ‘doped’ with copper or silver. | Not microbicidal; may be expensive; scale up to large surfaces questionable; not feasible to retrofit. |
| Diamond-like carbon (DLC) films | Manufactured-in | Reduces deposition; can be ‘doped’ with copper or silver. | Not microbicidal; likely to be expensive; feasibility of scale up to large surfaces questionable; not feasible to retrofit. |
There are some other options not listed in the table, that could be considered candidates for antimicrobial surfaces, although they are currently at an early stage of development, including:
- Negative air ionization to repel bacteria from surfaces.10
- Enzymes immobilized on surfaces.11
- Bacteriophages immobilized on surfaces.12
There is an impressive and rapidly emerging evidence-base for copper surfaces.13 The implementation of copper high-touch surfaces, which have a continuous biocidal action, results in a reduction in contamination and may reduce transmission.14-16 However, copper is expensive, difficult to retrofit and durability may be questionable.13,17 Thus, an effective disinfectant with a residual activity that does not compromise staff or patient safety or promote the development of reduced susceptibility is desirable. Several candidate disinfectants that have residual activity with a variety of active chemicals have emerged.18-22 These can be delivered through pre-existing cleaning and disinfection arrangements at little or no extra cost. However, there is very little published data on the microbiological or clinical impact of disinfectants with residual activity. A number of recent study suggest that promising in vitro activity may not translate into “real-world” impact: a recent study by Boyce et al. found that two organosilane products simply did not work as intended when applied to surfaces in a US hospital.22
During my research for this post, I came across a very useful presentation by Peter Hoffman from Public Health England, which can be downloaded here. Taking some of his ideas, plus a few of my own, the following points for discussion emerge:
- Which is the optimal deployment mode – antimicrobial agents that are manufactured in or periodically applied, or ways to make the surface physically less able to support contamination or easier to clean?
- If periodic application is selected, how frequently is a fresh application required (i.e. how durable is the antimicrobial coating)?
- Which surfaces should be made antimicrobial? It’s probably not feasible to do them all, particular for antimicrobial options that need to be manufactured in.
- Surfaces in hospitals are often dirty (obviously); it’s not clear how much the presence of organic matter would interfere with the activity of antimicrobial surfaces. Clearly, antimicrobial surfaces do not obviate the need for careful attention to hospital cleaning and disinfection. In fact, their continued effectiveness depends on it.
- The deposition of contamination and potential acquisition of contamination through contact with surfaces often occurs in quick succession, so antimicrobial surfaces with a contact time measure in minutes (rather than seconds) may be too slow to be useful.
- C. difficile spores represent a real challenge to antimicrobial surfaces. Copper seems to get closest to demonstrating inactivation, but even here data are somewhat equivocal.23 Could introducing an antimicrobial surface that is not effective against C. difficile “squeeze the balloon” and provide a selective advantage to C. difficile?
- How effective will antimicrobial surfaces that rely on an active agent leaching from surfaces be in a dry environment?
- How do we test – and compare efficacy – of antimicrobial surfaces? A standardized test has been proposed,24 but not yet adopted widely. Importantly, this methodology specifies an aerosol deposition of microbes whereas other proposed methodologies specify the deposition of microbes in a liquid suspension. Testing the ‘wet’ deposition of microbes may overestimate the antimicrobial potential of the surfaces, which would usually be challenged with dry deposition in the real world.
- Much of the literature for antimicrobial surfaces is published in materials science journals, as illustrated in this useful review by Page et al.25 I, for one, find this pretty difficult to access; as a healthcare scientist, it’s a new and daunting language to learn.
- The cost, and cost-effectiveness of implementing antimicrobial surfaces in the healthcare setting has not been rigorously assessed.
There’s a plethora of potential options and approaches to make a hospital surface ‘antimicrobial’. Copper is leading the way as a candidate, although other options are available. Making a surface less able to support contamination in the first place, and / or easier to clean is another tempting option, particularly if this can be combined with a level of antimicrobial activity. Finding and evaluating the optimal antimicrobial surface will require a multidisciplinary approach, requiring industrial partners, materials scientists, healthcare scientists and epidemiologists to refine and test the available options. More studies in the clinical setting, ultimately including those with a clinical outcome, are required.
Photo credit: Benjamin Hall.
References
1. Mayfield JL, Leet T, Miller J, Mundy LM. Environmental control to reduce transmission of Clostridium difficile. Clin Infect Dis 2000; 31: 995-1000.
2. Donskey CJ. Does improving surface cleaning and disinfection reduce health care-associated infections? Am J Infect Control 2013; 41: S12-19.
3. McMullen KM, Zack J, Coopersmith CM, Kollef M, Dubberke E, Warren DK. Use of hypochlorite solution to decrease rates of Clostridium difficile-associated diarrhea. Infection Control and Hospital Epidemiology 2007; 28: 205-207.
4. Boyce JM, Havill NL, Otter JA et al. Impact of hydrogen peroxide vapor room decontamination on Clostridium difficile environmental contamination and transmission in a healthcare setting. Infect Control Hosp Epidemiol 2008; 29: 723-729.
5. Orenstein R, Aronhalt KC, McManus JE, Jr., Fedraw LA. A targeted strategy to wipe out Clostridium difficile. Infect Control Hosp Epidemiol 2011; 32: 1137-1139.
6. Hayden MK, Bonten MJ, Blom DW, Lyle EA, van de Vijver DA, Weinstein RA. Reduction in acquisition of vancomycin-resistant enterococcus after enforcement of routine environmental cleaning measures. Clin Infect Dis 2006; 42: 1552-1560.
7. Hardy KJ, Gossain S, Henderson N et al. Rapid recontamination with MRSA of the environment of an intensive care unit after decontamination with hydrogen peroxide vapour. J Hosp Infect 2007; 66: 360-368.
8. Otter JA, Cummins M, Ahmad F, van Tonder C, Drabu YJ. Assessing the biological efficacy and rate of recontamination following hydrogen peroxide vapour decontamination. J Hosp Infect 2007; 67: 182-188.
9. Humphreys H. Self-disinfecting and Microbiocide-Impregnated Surfaces and Fabrics: What Potential in Interrupting the Spread of Healthcare-Associated Infection? Clin Infect Dis 2013;
10. Shepherd SJ, Beggs CB, Smith CF, Kerr KG, Noakes CJ, Sleigh PA. Effect of negative air ions on the potential for bacterial contamination of plastic medical equipment. BMC Infect Dis 2010; 10: 92.
11. Pangule RC, Brooks SJ, Dinu CZ et al. Antistaphylococcal nanocomposite films based on enzyme-nanotube conjugates. ACS Nano 2010; 4: 3993-4000.
12. Markoishvili K, Tsitlanadze G, Katsarava R, Morris JG, Jr., Sulakvelidze A. A novel sustained-release matrix based on biodegradable poly(ester amide)s and impregnated with bacteriophages and an antibiotic shows promise in management of infected venous stasis ulcers and other poorly healing wounds. Int J Dermatol 2002; 41: 453-458.
13. O’Gorman J, Humphreys H. Application of copper to prevent and control infection. Where are we now? J Hosp Infect 2012; 81: 217-223.
14. Salgado CD, Sepkowitz KA, John JF et al. Copper surfaces reduce the rate of healthcare-acquired infections in the intensive care unit. Infect Control Hosp Epidemiol 2013; 34: 479-486.
15. Schmidt MG, Attaway HH, Sharpe PA et al. Sustained reduction of microbial burden on common hospital surfaces through introduction of copper. J Clin Microbiol 2012; 50: 2217-2223.
16. Rai S, Hirsch BE, Attaway HH et al. Evaluation of the antimicrobial properties of copper surfaces in an outpatient infectious disease practice. Infect Control Hosp Epidemiol 2012; 33: 200-201.
17. Weber DJ, Rutala WA. Self-disinfecting surfaces. Infect Control Hosp Epidemiol 2012; 33: 10-13.
18. Keward J. Disinfectants in health care: finding an alternative to chlorine dioxide. Br J Nurs 2013; 22: 926, 928-932.
19. Hedin G, Rynback J, Lore B. Reduction of bacterial surface contamination in the hospital environment by application of a new product with persistent effect. J Hosp Infect 2010; 75: 112-115.
20. Baxa D, Shetron-Rama L, Golembieski M et al. In vitro evaluation of a novel process for reducing bacterial contamination of environmental surfaces. Am J Infect Control 2011; 39: 483-487.
21. Brady MJ, Lisay CM, Yurkovetskiy AV, Sawan SP. Persistent silver disinfectant for the environmental control of pathogenic bacteria. Am J Infect Control 2003; 31: 208-214.
22. Boyce JM, Havill NL, Guercia KA, Schweon SJ, Moore BA. Evaluation of two organosilane products for sustained antimicrobial activity on high-touch surfaces in patient rooms. Am J Infect Control 2014;
23. Wheeldon LJ, Worthington T, Lambert PA, Hilton AC, Lowden CJ, Elliott TS. Antimicrobial efficacy of copper surfaces against spores and vegetative cells of Clostridium difficile: the germination theory. J Antimicrob Chemother 2008; 62: 522-525.
24. Ojeil M, Jermann C, Holah J, Denyer SP, Maillard JY. Evaluation of new in vitro efficacy test for antimicrobial surface activity reflecting UK hospital conditions. J Hosp Infect 2013; 85: 274-281.
25. Page K, Wilson M, Parkin IP. Antimicrobial surfaces and their potential in reducing the role of the inanimate environment in the incidence of hospital-acquired infections J Mat Chem 2009; 19: 3819-3831.
Three good reasons why not to “copperize” your hospital surfaces
I recently received an email from the Copper Development Association entitled “Five Good Reasons to Install Antimicrobial Copper Touch Surfaces”. The five reasons are as follows:
- “Continuous and significant bioburden reduction, 24/7.
- Improved patient outcomes.
- A supplement to standard hygiene practices.
- Simple, cost-effective intervention.
- Payback in less than one year.”
I agree with all of these points in principle, and like the recently published copper study a lot, but I recently had two experiences that gave me three good reasons why not to “copperize” a hospital room.
Firstly, I was kindly given a copper pen at a conference. I’ve had it for a few months now and it’s beginning to look slightly the worse for wear (note the tarnishing where my grubby mits have been holding it, and the bright shiny part that has had less exposure to air underneath the swivel top). Is this how a bedrail would look after a few months of use?

Secondly, the pen works well but my hands smell of metal after using it. Would it be the same after touching my copper bedside table?
Thirdly, we had a new boiler installed last year resulting in a small pile of scrap copper pipes. I eventually got around to taking the copper pipes to the scrap metal merchant last weekend, expecting to get nothing for them and he gave me £50. So, exactly how much would it cost to “copperize” a hospital room, and would you really see ‘payback in less than one year’?
I appreciate that much of this may have to do with the composition of the copper alloy. I would imagine that reducing the amount of copper in the alloy would mean lower cost, less smell and less tarnishing. However, it would also reduce the ability to inactivate microbes deposited on the surfaces, so the research data really only applies to the composition of the copper alloy in the items that were tested. Also, there’s been some academic criticism of the copper study on the Controversies in Hospital Infection Prevention blog which is worth reading.
There are still a lot of questions around the implementation of copper surfaces in hospital rooms, and there are other options to consider. But I do think we should be thinking seriously about evaluating the clinical impact and cost-benefit of implementing antimicrobial surfaces.
Can the introduction of 6 copper items into ICU rooms really reduce the rate of HAI by >50%?
The recent article by Salgado et al.in the ICHE special edition is the long-awaited copper study: a multi-centre evaluation of the clinical impact of introducing 6 copper alloy high-touch sites into the rooms of patients on three ICUs. I’ve been looking forward to getting my hands on this study for some time!

Patients (n=614 following exclusions) were randomized to intervention ‘copper’ rooms and control ‘non-copper’ rooms in three USA ICUs over an 11 month period. The only difference between the rooms was the presence of six items made of copper alloy, comprising bedrails, overbed tables, IV poles and visitor chair arms in all rooms and the nurse call button, computer mouse, computer palm rest and rim of a touch-screen monitor in other rooms.
Patients admitted to copper rooms were significantly less likely to acquire healthcare-associated infection (HAI) or colonization with MRSA / VRE (Figure).
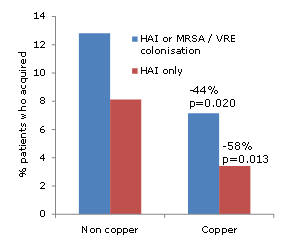
Figure: difference in acquisition rate between patients admitted to ‘copper’ or ‘non-copper’ rooms
The authors also make an interesting association between the degree of contamination in patient rooms and the risk of acquisition. However, since sampling was performed weekly regardless of a patient’s infection or colonization status, it is not possible to determine whether this association is causal or simply due to the fact that infected / colonized patients are likely to shed more bacteria into the hospital environment.
The study team should be commended for the careful design and attention to detail in the execution of the study. For example, they performed a daily census of the items in the study to determine exactly who was exposed to copper surfaces, and for how long. This indicated that only half of the patients in ‘copper’ rooms were exposed to all six copper items for the duration of their stay, and 13% of patients in the ‘non-copper’ arm were exposed to some copper items during their stay. It’s important to note that the analysis was performed on an ‘intention to treat’ population, i.e. all patients randomized to the two groups, regardless of which items they were actually exposed to. It would have been interesting to see a sub-analysis on the ‘per protocol’ population (i.e. those patients admitted to ‘copper’ rooms and exposed to all six copper items vs. those patients admitted to ‘non-copper’ rooms and exposed to no copper items). Also, I’m not sure why they chose to analysis % acquisition rather than a comparison of rates between the groups. And then there’s the salary support and grant funding to some authors (not directly related to this study) from the Copper Development Association. Notwithstanding these limitations, it does seem that the introduction of copper high-touch surfaces does reduce the transmission of hospital pathogens.
The scale of the difference is incredible. And I mean just that. It lacks credibility. Many will dismiss the study simply because of the scale of the difference between the groups. So, can the introduction of 6 copper items into ICU rooms really reduce the rate of HAI by >50%?
The degree to which contaminated surfaces contribute to the transmission of pathogens is up for debate. I was asked to give a talk at APIC 2012 on the role of the environment. Prior to the talk, I asked the expert faculty a question: ‘What is your estimation of the % of allC. difficile transmission in hospitals that is mediated, directly or indirectly, by contamination of the inanimate environment?’ The answers ranged from 25-75%, reflecting the uncertainty on this issue.
A recently published study by Johns Hopkins provides some illuminating findings (albeit indirectly). Extrapolating unadjusted acquisition rates from all study cohorts indicates that if rooms had been disinfected using hydrogen peroxide vapour (HPV) after every discharge, the overall rate of acquisition of MDROs would have been halved. Whilst it’s not feasible to disinfect all rooms using HPV at patient discharge, this does add some weight to the scale of the reduction identified in this copper study.
It seems that the introduction of a handful of copper alloy high-touch sites had a profound impact on HAI rates. On reflection, I do believe it possible that the scale of reduction in study is “real”. However, questions remain over the practicality and durability of the widespread adoption of copper alloy surfaces in healthcare.
Article citation:
