I recently received an email from the Copper Development Association entitled “Five Good Reasons to Install Antimicrobial Copper Touch Surfaces”. The five reasons are as follows:
- “Continuous and significant bioburden reduction, 24/7.
- Improved patient outcomes.
- A supplement to standard hygiene practices.
- Simple, cost-effective intervention.
- Payback in less than one year.”
I agree with all of these points in principle, and like the recently published copper study a lot, but I recently had two experiences that gave me three good reasons why not to “copperize” a hospital room.
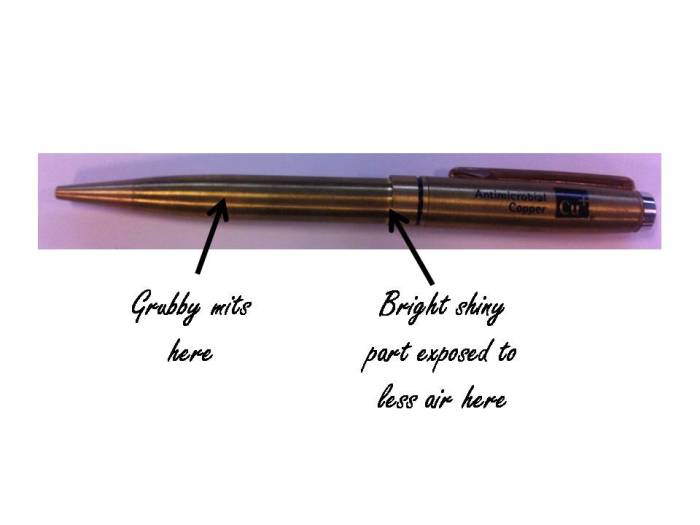
Firstly, I was kindly given a copper pen at a conference. I’ve had it for a few months now and it’s beginning to look slightly the worse for wear (note the tarnishing where my grubby mits have been holding it, and the bright shiny part that has had less exposure to air underneath the swivel top). Is this how a bedrail would look after a few months of use?
Secondly, the pen works well but my hands smell of metal after using it. Would it be the same after touching my copper bedside table?
Thirdly, we had a new boiler installed last year resulting in a small pile of scrap copper pipes. I eventually got around to taking the copper pipes to the scrap metal merchant last weekend, expecting to get nothing for them and he gave me £50. So, exactly how much would it cost to “copperize” a hospital room, and would you really see ‘payback in less than one year’?
I appreciate that much of this may have to do with the composition of the copper alloy. I would imagine that reducing the amount of copper in the alloy would mean lower cost, less smell and less tarnishing. However, it would also reduce the ability to inactivate microbes deposited on the surfaces, so the research data really only applies to the composition of the copper alloy in the items that were tested. Also, there’s been some academic criticism of the copper study on the Controversies in Hospital Infection Prevention blog which is worth reading.
There are still a lot of questions around the implementation of copper surfaces in hospital rooms, and there are other options to consider. But I do think we should be thinking seriously about evaluating the clinical impact and cost-benefit of implementing antimicrobial surfaces.



