Yet another study has just appeared in AJIC ‘In Press’ that reports on a long-term, discontinuous ‘outbreak’ of Pseudomonas (see http://www.ajicjournal.org/article/S0196-6553%2815%2900138-8/abstract). Once again everything points back to the sinks in the unit and a reusable washbasin for hairwashing. So all back to water and practice issues around it. Water is dangerous you know, nearly 100% of murderers and theives have consumed it in the 24 hrs preceding their crimes and it is the leading cause of drowning. Seriously though, wouldn’t we expect to find Pseudomonas in a sink trap? It is how it gets to the patient that is the issue. I was in a hospital overseas recently where mop-heads were conveniently placed either side of the sink to soak up splashes from the basin. So, why were there splashes? The sink trap was just a hole and so the staff had placed big grilles over the bottom of the sink to prevent items going down and blocking the sink. Turning on the tap produced a very attractive set of fountains, a bit like at the end of ‘Oceans 11’. Nuff said
Year: 2015
Do you know your CRE from your CRAB?
I gave a talk today at a meeting on combating carbapenem-resistant organisms. My angle was to clearly differentiate the epidemiology of the Enterobacteriaceae (i.e. CRE) from the non-fermenters (most importantly carbapenem-resistant A. baumannii – CRAB), and you can download my slides here.
I’ve blogged before about how confusing the terminology surrounding multidrug-resistant Gram-negative rods has become. Non-expert healthcare workers have little chance in distinguishing CRE from CPE from CRO from CPO. So we need to help them by developing some clear terminology, given the gulf in epidemiology between CRE and CRAB (see below).
CRE and CRAB are like apples and pears: they share some basic microbiology but that’s about where the comparison ends!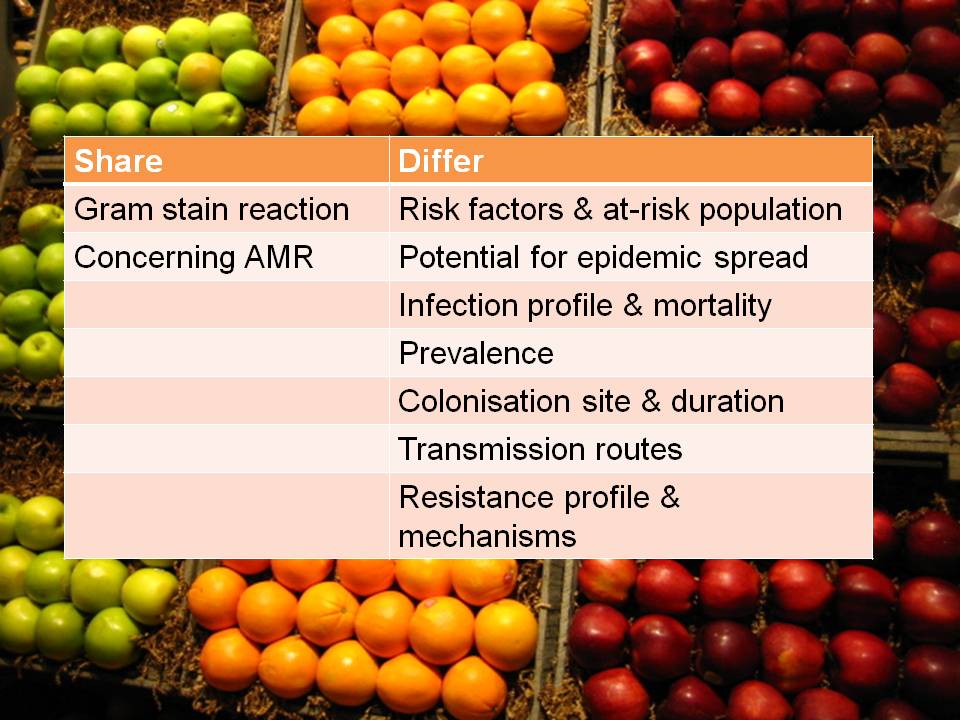
So, I think we should talk in terms of CRE (and CPE for confirmed carbapenemase carriers), and CRNF (or CRAB for A. baumannii and CRPA for P. aeruginosa). I don’t think that CRO is a useful term – in fact, I find it rather confusing. Carbapenem resistance in Enterobacteriaceae (CRE) and A. baumannii (CRAB) are both emerging problems, but they are not the same problem.
And we wonder why E. coli bacteraemia is rising..
Leicester incontinence sufferer ‘too frightened’ to drink water – http://www.bbc.co.uk/news/uk-england-leicestershire-32222349
Is there a link between gram-negative bacteraemia and hydration? Evidence a bit thin but I find it highly plausible, especially given the papers from all over the planet demonstrating seasonality. Pads vs antibiotics. No brainer
Rescuscitation
Time to wake this sleeping blog up I think. Plenty of material out there. I’m just back from a trip to Asia, including the APSIC meeting in Taiwan. What struck me was the huge amount of interest in the environment. The meeting kicked off with a keynote on the subject and looking through the programme there was a session on environmental contamination in virtually every concurrent. Acinetobacter is the primary concern and they’ve not got started on C. difficile yet (mainly helped by not looking for it.. I wish I’d thought of that)
How big is C. difficile infection in the USA?
 The New England Journal of Medicine recently published an article evaluating the burden of CDI in the USA. The huge CDC-led initiative collected data from 10 geographically distinct regions, identifying more than 15,000 cases. Around two-thirds of cases were classified as healthcare-associated (although only 25% were hospital-onset). This means that, prima facie, a third of CDI cases were community-associated. I find this proportion difficult to believe: I strongly suspect that many of these cases would have had healthcare-associated risk factors if the team were able to look hard enough. For example, they used a fairly standard 12 week look-back period to evaluate previous hospitalisation, but how would the data look if they’d used 12 months? Also, it’s usually only possible to evaluate previous hospitalisation in a single healthcare system, but many patients commute between various healthcare systems. The authors acknowledge in the discussion that this designation of “community-acquired” may be inaccurate based on the finding from a previous study whether healthcare-associated risk factors were identified in most patients, but only be a detailed phone interview.
The New England Journal of Medicine recently published an article evaluating the burden of CDI in the USA. The huge CDC-led initiative collected data from 10 geographically distinct regions, identifying more than 15,000 cases. Around two-thirds of cases were classified as healthcare-associated (although only 25% were hospital-onset). This means that, prima facie, a third of CDI cases were community-associated. I find this proportion difficult to believe: I strongly suspect that many of these cases would have had healthcare-associated risk factors if the team were able to look hard enough. For example, they used a fairly standard 12 week look-back period to evaluate previous hospitalisation, but how would the data look if they’d used 12 months? Also, it’s usually only possible to evaluate previous hospitalisation in a single healthcare system, but many patients commute between various healthcare systems. The authors acknowledge in the discussion that this designation of “community-acquired” may be inaccurate based on the finding from a previous study whether healthcare-associated risk factors were identified in most patients, but only be a detailed phone interview.
Scaling up from the figures from the 10 regions, national estimates were around 500,000 cases and 29,000 deaths due to CDI per annum in the US. This estimate is approximately double previous estimates for the national CDI burden in the USA, probably reflecting the adoption of molecular methods for the detection of CDI. This scaling up included an interesting statistical adjustment to see how prevalence varied depending on how many sites use sensitive molecular methods to detect CDI.
A sub-study included the culture of C. difficile from 1625 patients. More than 15% of stool specimens from patients diagnosed as CDI failed to grow C. difficile, probably illustrating the limitations of culture methods more than anything else. NAP1 (027) represented around half of cases, and was significantly more common in healthcare-associated CDI. I think it’s fair to say that the initial fears that NAP1 was a super-strain have been allayed by the fact that it’s now so common and there hasn’t been a surge in CDI mortality.
Finally, around 21% of healthcare-associated cases suffered at least one recurrence. Thus, there is a real need to the roll out of the uber successful faecal microbiota transplantation for recurrent CDI. In fact, there should be around 70,000 faecal microbiota transplantations each year in the US right now (500,000 x 0.66 x 0.21); I suspect there are far fewer.
Journal of Hospital Infection Special Edition on the 2014 Healthcare Infection Society (HIS) Conference

JHI have published a Special Edition featuring write-up from the 2014 HIS Conference (you can see my reflections from HIS here).
- The Special Edition kicks off with a thoughtful editorial by the guest editor Dr Mark Walker, in praise of enthusiasts and in defence of conferences.
- Dr Seto’s Lowbury lecture exploring facts and myths around airborne transmission.
- My overview of trends in the infection prevention and control literature since the 2012 HIS conference (there’s been one trend that trumps all other trends: Ebola). You can download the slides and see a recording of this talk here. Also, Dr Jim Gray’s take on future trends.
- Updates on multidrug-resistant Gram-negative bacteria, including the importance of globalization, experiences of controlling CRE and Acinetobacter outbreaks, the role of antibiotic prophylaxis in driving the problem.
- Antibiotic stewardship is covered from a couple of angles, including a surgeons’ perspective and long-term care facilities in Ireland.
- Several articles address surveillance, including the role of ‘data warehousing’, integration of electronic systems, and surveillance of ventriculitis following neurosurgery.
- Not much on the role of the environment, although Dr Frederic Barbut provides an overview of methods to eradicate (or not!) C. difficile from the hospital environment.
- State-of-the-art updates on norovirus, Candida, influenza (specifically the role of point-of-care testing), P. aeruginosa, cystic fibrosis, and HCAI in neonates.
- Management and organisational factors are reviewed, and other articles address assessment and public-reporting, root-cause analysis, human factors, training, and current knowledge.
- Finally, and importantly, the impact of the recession on HCAI is reviewed. The recession has hit hard in Ireland, where this article was penned from, but the article at least offers some useful pragmatic coping strategies!
I’m all for special editions, and I think that JHI should do more of them. I know that compiling this Special Edition has been a considerable undertaking for the Journal, but well worth the effort: it’s a very useful read. Particular thanks to Dr Mark Walker who was the editor for this Special Edition, and to Dr Jenny Child who initiated it.
Over the top and into the trenches
 After 12 years working for Bioquell (and part-time at Guy’s and St. Thomas’ / King’s College London since commencing my PhD in 2005), it’s time for me to move onto pastures new. Next week I’ll start working in a leadership role in Infection Prevention and Control at Imperial College NHS Trust in London. It’s a very exciting move for me and I can’t wait to get going. I thought that now would be a good time to reflect on the water under the bridge of the last decade or so (and I hope you’ll forgive my self-indulgence).
After 12 years working for Bioquell (and part-time at Guy’s and St. Thomas’ / King’s College London since commencing my PhD in 2005), it’s time for me to move onto pastures new. Next week I’ll start working in a leadership role in Infection Prevention and Control at Imperial College NHS Trust in London. It’s a very exciting move for me and I can’t wait to get going. I thought that now would be a good time to reflect on the water under the bridge of the last decade or so (and I hope you’ll forgive my self-indulgence).
Over the last decade, the rate of MRSA and C. difficile infection (CDI) in the UK have fallen dramatically.1,2 At the peak of the MRSA epidemic in the early 2000s, there were more than 2000 MRSA bloodstream infections per quarter in England; now there are 10-fold less.2 It’s not certain how this has been achieved, but a combination of factors, including increased governmental focus, are likely responsible. Whilst MRSA is now rare in the UK this is not the case in other European countries and in many other parts of the world, where MRSA remains common.3
In recent years, a new and more troublesome bacterial threat has emerged: carbapenem-resistant Enterobacteriaceae (CRE).4 CRE present the “triple threat” of high levels of antibiotic resistance (including pan-drug resistant strains against which no antibiotics are left), severe clinical consequences (around half of patients with a CRE bloodstream infection will die), and the potential for rapid regional and national spread (illustrated by national outbreaks in Italy, Greece and Israel).4-6 CRE have been described as “nightmare bacteria” by the US CDC and have prompted unprecedented action from CDC, Public Health England (PHE) and other public health agencies, including a national Patient Safety Alert and a letter to all hospital Chief Executives in the UK to ensure that new CRE guidelines are implemented.7,8
CRE diagnosis: current status
I had the opportunity to ask the audience how they were detecting CRE in their diagnostic clinical labs during a talk last week. It was an audience of around 50 laboratory and clinical folk, mainly from the UK but a few from continental Europe. And here’s what I found:
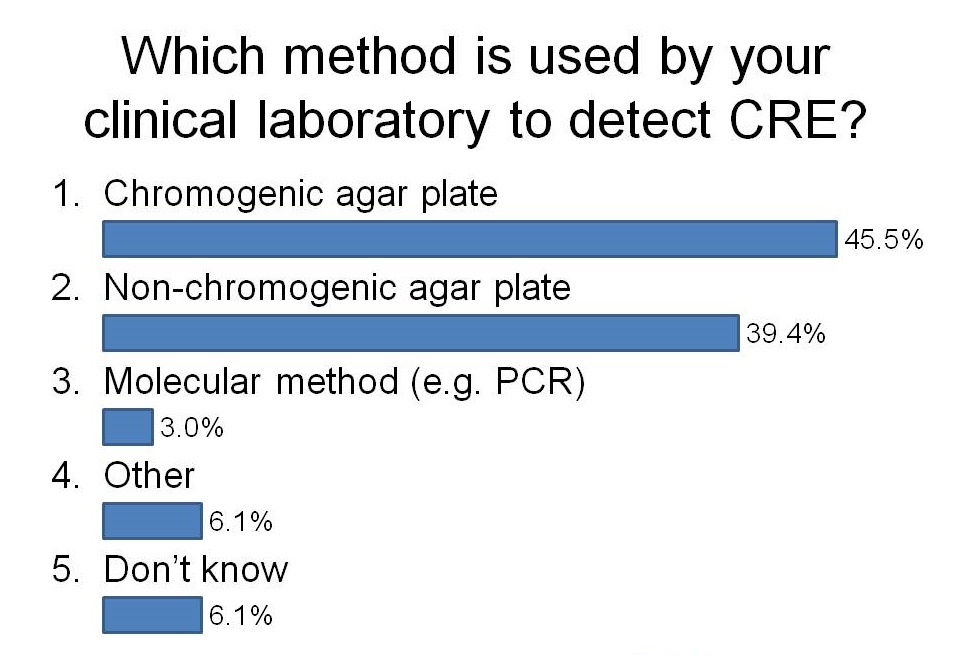
I was a little surprised that more labs have switched to using chromogeneic agar plates than use non-chorogeneic agar plates. In the case of our lab in London, we are currently using non-chromogenic media for clinical samples, but in the process of evaluating chromogenic media. Although the purchase costs of chromogenic media are higher, they are more sensitive and substantially reduce the amount of time required to confirm a negative or positive culture, so I suspect they actually work out cheaper when you factor in labour costs.
I was not surprised that so few labs are using PCR. The costs are considerably higher but turnaround time is faster and they are more sensitive. There are now a number of PCRs on the market for the detect of CRE direct from rectal swabs (e.g. Checkpoints and Cepheid). We are currently in the process of evaluating the Checkpoints assay and after sharing our preliminary data, this was the feeling in the room about using PCR to detect CRE:

I think I’ll leave it there for now…
Diagnosis of CRE: time to throw away those agar plates?
CRE are an emerging threat to healthcare systems worldwide. Most guidelines recommend screening and isolation of carriers. But relying on conventional agar-based culture presents a dual threat of poor sensitivity (depending on which method is used) and slow turnaround time, with a minimum overnight incubation before a presumptive positive result. PCR solves both of these problems – but at a cost. I gave a talk today at a BD seminar considering whether it’s time to switch to PCR diagnostics for the detection of CRE. You can download my slides here. (The title of the talk “Time to throw away those agar plates” was inspired by a talk by Dr Dan Diekema at a recent SHEA conference.)
There are a number of options for CRE screening, summarized in the flow chart below:
Flow chart: Overview of laboratory methods for the diagnosis of CRE. (To be precise, throughout the blog I really mean CPE most of the time, but I’m using CRE for consistency with other blogs…)
The English MRSA Miracle
If, in 2004, I’d told an MRSA expert that there would be around only 200 MRSA bloodstream infections (BSI) per quarter in England throughout 2014 they’d have laughed out loud. This is because, back in 2004, there were sometimes more than 100 MRSA BSI per month in some London hospitals (and around 2000 per quarter nationally), combined with a general perception that only around 30% of MRSA BSI are preventable. How wrong we were.
The reduction of MRSA BSI in England has been dramatic, with a reduction in the region of 90% achieved over a 5 year period. I was asked to speak on “The English MRSA Miracle” at a conference in Portugal today, so thought I’d share my thoughts. You can download my slides here.
It’s difficult to pin down exactly what is behind the ‘MRSA Miracle’ since quite a number of interventions occurred at more or less the same time (Figure 1):
Figure 1: National interventions aimed at reducing MRSA BSI.
Some have postulated that the national cleanyourhands campaign is responsible for the dramatic success. Indeed, there is a BMJ study that makes this case, showing that the national significant increase in the use of soap and water and alcohol gel correlated with the reduction in MRSA BSI. However, I contend that this can’t be the case because what has happened to the rate of MSSA and E. coli BSI over the same period? Nothing – no reduction whatsoever. If increases in hand hygiene compliance really do explain the reduction in MRSA BSI, then they should also reduce the rate of MSSA BSI (unless the increase in hand hygiene compliance only occurred after caring for MRSA patients, which seems unlikely).
There’s a more important epidemiological point here though. High-school tells us to change one variable at a time in science experiments. And yet in this case multiple variables were modified, so it’s not good science to try to pin the reduction to a single intervention, no matter how strong the correlation. (I should add that the authors of the BMJ study do qualify their findings to a degree: ‘National interventions for infection control undertaken in the context of a high profile political drive can reduce selected healthcare associated infections.’)
There has been much discussion about whether we should be investing in a universal or targeted approach to infection control. The failure of improved hand hygiene to make any impact on MSSA BSI suggests that targeted interventions are behind the reduction in MRSA. So what targeted interventions were implemented that may have contributed to the decline? MRSA reduction targets were introduced in 2004, a series of ‘high-impact interventions’ focused mainly on good line care in 2006 and revised national guidelines in 2006 (including targeted screening, isolation and decolonization) all contributed to a surge of interested infection control. Infection control teams doubled in size. Infection control training became part of mandatory induction programmes. And hospital chief executives began personally telephoning infection control to check “how many MRSA BSIs” they had left.
The ‘English MRSA Miracle’ has not been matched in most parts of Europe, except in France, which has had a rather more steady ‘MRSA Miracle’ of its own (Figure 2).
Figure 2: Rate of methicillin-resistance in invasive S. aureus infections, from EARS-Net.
What is behind the failure of most European countries in controlling MRSA? The barriers are multifactorial, but include high levels of antibiotic use, a lack of single rooms for isolating patients, infection control staffing, and, of course, crippling national debt (Figure 3).
Figure 3: Barriers to infection prevention and control in Europe.
If the English MRSA Miracle is to be replicated across Europe, it will take concerted national initiatives to raise the profile of infection control, combined with considerable investment, which is challenging in these times of austerity.
