Hand Hygiene and Self-Protection
Hand Hygiene and Self-Protection
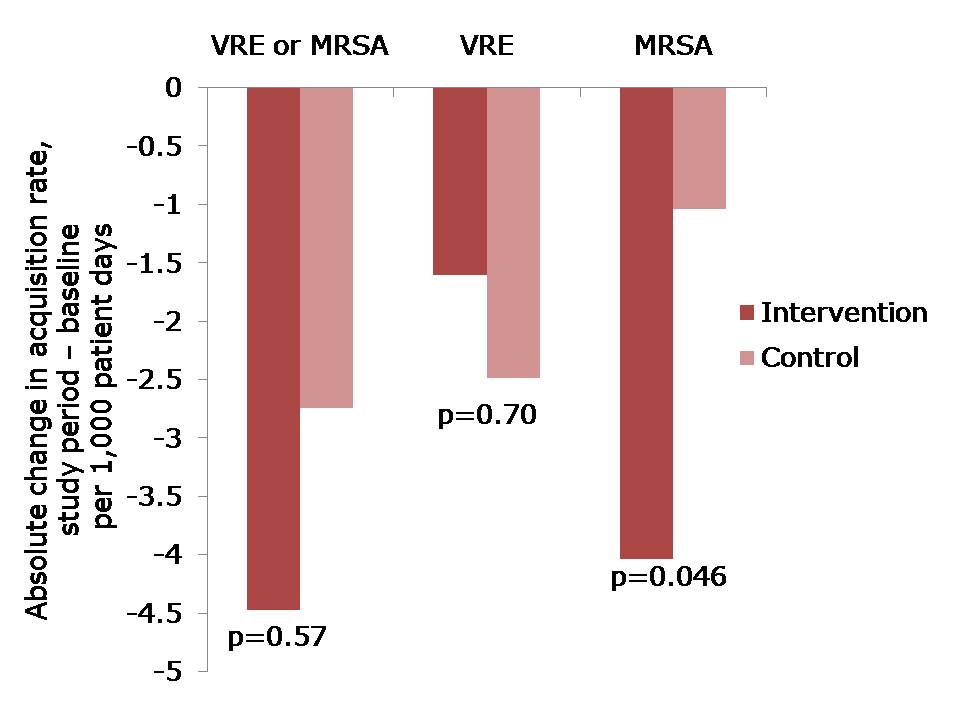
Guest blogger Carolyn Dawson (bio below) writes: The BUGG study provides support for the concept of self-protection in hand hygiene through its findings that healthcare professionals were more likely to perform hand hygiene after leaving a patient room than upon entry (mean compliance at room exit vs. entry in intervention universal glove and gown group: 78.3% vs. 56.1%, respectively; mean compliance control group: 50.2% vs. 62.9%, respectively). This may suggest a stronger awareness of contamination occurring on the hands during patient interaction than of contamination having occurred prior to patient contact. It may also indicate a higher prioritisation of the implications of contamination acquired during, rather than prior to, patient contact.
The discussion here is how such self-protection themes may affect the concept of universal glove use providing a benefit to patient safety. The “urgh” factor provides a simple phrase to represent instinctive hand hygiene drivers, both at times when hands become physically soiled and when they are in contact with things which have an “emotionally dirty” association (e.g. armpits, clean bedpans) (based on Whitby et al., 2006). The “urgh” factor has been shown to increase likelihood of hand hygiene occurring in clinical practice (my research).
The “urgh” factor can be useful for driving hand hygiene: despite other pressing variables, such as time and workload, this instinctive self-protective driver increases the likelihood that hand hygiene will still occur on some occasions, providing the related patient and healthcare professional safety benefits. But it also means that there is less of a psychological driver for hand hygiene following contact with things that are perceived as “clean” but may be as contaminated as perceived “dirty” items.
Glove use reduces the “urgh” factor
The use of gloves (including inappropriate/over-use) has been shown to be driven by themes including disgust and fear (e.g. Wilson et al, 2013), suggesting their use leads to a feeling of security, reducing this “urgh” factor. Therefore, one could expect that activities previously resulting in high levels of hand hygiene would be affected by the adoption of universal glove use, as the “urgh” factor influence is reduced. In other words, if you are wearing gloves, you are less likely to feel repulsed by touching something you previously would have, and thus, in turn, are less likely to perform hand hygiene. Glove use is no substitute for effective hand hygiene, which should be performed both before and after gloves are used, and at specific points during patient care (RCN 2012).
For example: imagine moving from changing a catheter bag, to cleaning a wound. Both hand hygiene and the changing of gloves must be performed. With respect to the “urgh” factor, one could expect that instinctive drivers would motivate hand hygiene in this example, as self-protective drivers lean towards decontamination after handling the catheter bag. However, when gloves are used these desires may be muted, leaving a stronger demand on the knowledge and skills of the healthcare professional to perform necessary hand hygiene and glove use protocol.
‘Correct’ and ‘Incorrect’ glove use
It is worth noting that the definition of ‘appropriate’ use of gloves is subjective, with different settings likely to adhere to different standards and guidelines. Thus, caution is required when discussing ‘correct’ and ‘incorrect’ use of gloves. There are, however, some less debatable examples where gloves are not recommended due to low risk of contamination (RCN 2012, Appendix 1), yet gloves are often used e.g. collecting equipment, writing notes (Flores and Pevalin, 2006).
The use of gloves for these activities combined with uninterrupted use of gloves (from one activity/area to another without removal – Girou et al., 2004), likely results in microbial cross-contamination via the surface of these gloves. Such activities provide no “urgh” factor safety net, therefore the need to change gloves and perform required hand hygiene requires conscious decisions from the healthcare professional, demanding cognitive input. Commenting on the misuse of gloves, Fuller et al. (2011) wrote: “the reality is that healthcare workers do not always clean their hands before donning gloves, that their hands pick up further organisms during high-risk contacts, and that hands are not always cleaned when the gloves are removed.” It seems likely that a move towards universal gloving would result in more inappropriate ‘continued use’ activities occurring.
Correct, not universal glove use
Such knowledge suggests that rather than looking towards universal gloving as a preventative strategy, continued focus should be turned towards ensuring current glove use is appropriate, seeking to harness the “urgh” factor safety net to drive hand hygiene compliance.
Carolyn Dawson Bio
I am about to submit a PhD dissertation on healthcare hand hygiene which explores the challenges faced in monitoring, measuring and providing feedback compliance data: the audit process. My research questions the potential of hand hygiene technologies (electronic surveillance) as an aid for this process, insisting that first their ‘Fitness-For-Purpose’ must be evaluated using recognised standards. The application of behavioural theory to understand how different activities may influence whether hand hygiene is executed is explored through pilot work on ‘Inherent’ and ‘Elective’ hand hygiene. This case study research has been carried out within an NHS acute setting, however application of the WHO “My 5 Moments for Hand Hygiene” as a core element allows the potential for future work to build upon this foundation outside the current setting. Prior to beginning my PhD I graduated with a BSc in Psychology and an MA from Warwick Business School, and then spent 6 years working for a global laser company as a Project Analyst.
Photo credit: CDC / Amanda Mills.