The latest ESPAUR report (2024–2025) paints a sobering picture of AMR in England. While prescribing practices have improved in some areas, the resistant infections are increasing, and new threats like Candidozyma auris are emerging.
Continue readingsurveillance
Avian influenza: it’s in the (waste)water
There is a sense of steadily building concern around avian influenza, remembering that an avian influenza outbreak would knock spots off COVID-19 (especially the modern variants) in terms of bad clinical outcomes. A letter in the NEJM relates wastewater surveillance in the state of Texas that has identified H5N1 avian influenza in all 10 cities in the surveillance programme since March 2024. This suggests that avian influenza is out there, and flying under the radar in animal populations. So, now would be a good time to dust down your pandemic influenza preparedness documents…
Continue readingHospital-onset COVID-19 (HOCI): a systematic review
As we get into gear to prepare for the next epidemic wave of COVID-19 affecting healthcare providers (hoping that it will not come), it’s a good time to review where we have got to with the surveillance of healthcare-associated COVID-19. Colleagues at Imperial have just published a systematic review of the latest literature on this important issue. Whilst uncertainties remain about surveillance definitions and exactly what “healthcare-associated COVID-19 infection” is, the message is clear that healthcare-providers must have in place clear and rapid systems for identifying healthcare-associated COVID-19 to prevent the spread of the SARS-CoV-2 virus in healthcare facilities.
Continue readingCPE: seek and ye shall find
We recently published a study in the Journal of Antimicrobial Chemotherapy relating the impact of introducing an enhanced testing* programme for CPE in London. (And yes, this is the first post for a while that isn’t on COVID-19!) Following an outbreak of NDM-producing Klebsiella pneumoniae affecting 40 patients in 2015 (published elsewhere, here and here), we ramped up our CPE testing programme. The number of patients carrying CPE increased substantially, from around 10 patients per month in June 2015 to around 50 per month in March 2018. However, the proportion of tests that were positive for CPE remained constant at around 0.4%, suggesting this was more effective carrier identification rather than a swelling pool of carriers per se; seek and ye shall find! Curiously, the majority of CPE identified were not linked in time and space with other CPE, suggested they represented a ground-swell of CPE coming into the hospital, rather than frequent in-hospital transmission. Also, the number of patients with CPE infections during the study period did not increase, which was reassuring.
CPE has landed in East London
The team at Barts Health, one of the largest NHS hospital groups in the country, has published the findings of a point prevalence screen of all inpatients for carbapenemase-producing organism (CPO) carriage. Overall, 30 (3.1%) of the 977 patient tested were carrying 35 different CPOs (all but one of which were CPE). Risk factors for CPO carriage included hospitalisation abroad, any hospitalisation, and overseas travel (especially to India, Pakistan, and Bangladesh). These findings help us to understand an emerging picture of CPO in the UK.
ESPAUR 2019: a snazzy facelift
The 2019 edition of the ESPAUR report has recently been published, including data up to and including 2018. The report is an excellent read – here’s a few summary points.
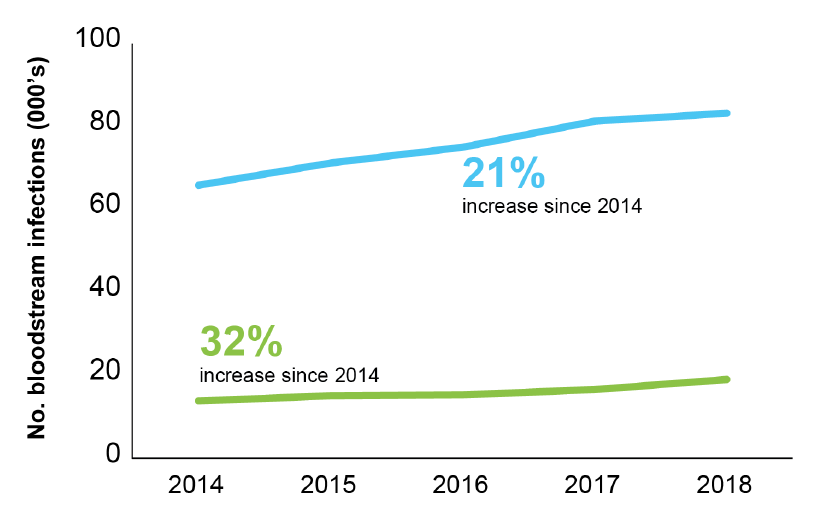
- There’s a series of lovely infographics at the start of the report. I gave myself a challenge: to select the one infographic that told the story of the report. I toyed with the one about a small but increasing number of CPE BSIs (aghhhhh!), and the stark grave-stone themed image of mortality related to carbapenemase-producers, but ended up with this one: alarmingly, the rate of BSI for the seven priority bacterial pathogens rose 22% between 2014 and 2018 to 145 per 100,000 population. (Around half of these were coli). And there’s a certain inexorability about the antimicrobial resistance trends included in this report, with a 32% increase in AMR BSIs comparing 2014 to 2018.
Figure: Trends in BSIs (blue line) and AMR BSIs (green line).
- There were more than 60k antibiotic resistant severe infections in 2018, <150 per day.
- Confirmed CPEs have topped 4k (but this is a gross underestimate of true prevalence). The report makes the case that the rarity of CPE BSIs (142 reported nationally) represents a success of prevention. This is probably true if we compare across the pond and towards the southern reaches of Europe. But difficult to be sure without a control (i.e. what would have happened without the national initiatives etc)? Also, reporting of CPE BSIs to PHE is voluntary and not mandatory, so there will be some degree of under-reporting.
- Related to this, only 50% of diagnostic labs have introduced methods to detect CPE locally. Which links closely with the change in surveillance system for CPEs going forwards – rather than manual voluntary reporting, locally confirmed CPEs will be reported automatically to PHE. However, if only 50% of diagnostic labs have appropriate methods, we’ll still end up under-reporting (but it will be more a more accurate picture than the current process provides).
- 30 day all-cause mortality of invasive CPE infections is 24% (along with the arresting gravestone-themed infographic)! Not sure how helpful it is to make a big point based on unadjusted mortality data…
- Overall consumption of antibiotics continues to decline. Consumption fell from 20 to 18 DDDs per 1,000 population per day between 2014 and 2018. However, consumption increased by 3% in hospitals over this period.
- There’s a nice section on Candida auris
- ESPAUR reports some good work and outcomes related to training, education, and awareness (e.g. Keep Antibiotics Working and Antibiotic Guardian).
- What a wonderful resource the AMR Fingertips module is: automated data from >90% of NHS laboratories on a range of AMR indicators at our…ahem…fingertips. I am one of the 15k users over the past three years. (As an aside, the volume of traffic is fairly low by popular website standards – but I guess it is somewhat niche!)
ESPAUR is a fantastic resource – it seems that this is the last ESPAUR report related to the UK AMR Strategy from 2013-2018, but I’m confident that ESPAUR will continue to report the successes and challenges of implementing the new five year action plan (from 2019-2024).
Make sure a (CPE) iceberg doesn’t sink your ship

An interesting modelling study has quantified the size of the CPE iceberg lurking under the water when CPE is only detected by clinical cultures and no active screening is done. And the CPE iceberg is larger than you may think!
Breaking the GLASS shroud around the global AMR crisis
WHO have published the first report of the Global Antimicrobial Resistance Surveillance System (GLASS) network. GLASS was launched a couple of years ago to try and address the massive black hole in our knowledge of global AMR resistance rates. The extensive report details progress to date, focussing on which countries have established surveillance systems, and how the initial data looks (which you can also view via an online database).
WHO is setting your IPC agenda

The World Health Organisation has updated its 2009 Guidelines on Core Components of Infection Prevention and Control Programmes. The report highlights eight ‘core components’ for IPC:
“HCAI”

I read a Controversies blog today, reflecting on a recent editorial suggesting that, because of frequent over-diagnosis, we should use quote marks every time we write “CAUTI” – and even use air quotes every time we say it! But why stop at CAUTI? Should we be talking about “CLABSI”, “CDI”, “SSI” and, well, any “HCAI” really?
