 Guest blogger Dr Evonne Curran (bio below) writes…
Guest blogger Dr Evonne Curran (bio below) writes…
Jon asked me to write on his blog about our column (‘#15: Carbapenemase-producing Enterobacteriaceae’). As he kindly accepted my offer to co-write a column, I accept his to write this blog. I am calling this blog (which contains only my personal views): ‘Carbapenem-resistant Enterobacteriaceae (CRE): so what should an infection prevention and control team do now?’.
The problems with CRE are numerous, and the different actions needed to control or at least delay its endemnicity are likewise legion; the task can seem insurmountable. The approach being taken at national and international level covers much of what is needed. The question for individual infection prevention and control teams (IPCTs) is this: where do you begin to protect a healthcare system that has little capacity (and in some cases little will) to start to solve a problem that essentially has yet to arrive, that has at least 6 names (none of which can be spelt with confidence) and is absent from the CEO’s performance monitoring agenda? The additional challenge for IPCTs is this: it will be difficult for those working in clinical areas to believe that for all the improvement in infection prevention and control that reduced MRSA and C. difficile, still more is required for this new microbiological-kid on the block.
If I were still part of a hospital based IPCT this is where I would start…..
- Give it a name and stick to it in all correspondence / education / awareness sessions;
- Succinctly provide the reasons as to why this should be on everyone’s radar;
- Take a high-reliability approach to strengthening your healthcare system;
- Involve patient advocates.
1) Give it a name and stick to it…
As mentioned in the column (and many times by Jon) there needs to be a name that we can a) all agree on and b) conveys to non-microbiology people the problem and its seriousness. We have to stop fighting about what it is: CPE, CRO, CPE etc, etc. I don’t know who is on (or how you get on) the micro-organism naming committee, but I am beginning to think they need to make it more democratic and involve people who don’t understand microbiology. There is no perfect name that will keep all microbiologists happy, so let’s stop trying to find one. It’s important that IPCTs have a short name that denotes this big problem and makes this consistent in all documentation. (See this previous blog by Jon for more info on nomenclature surrounding this issue.)
2) Succinctly provide the reasons as to why this should be on everyone’s radar
I offer the following as a succinct summary for why this should be on everyone’s radar:
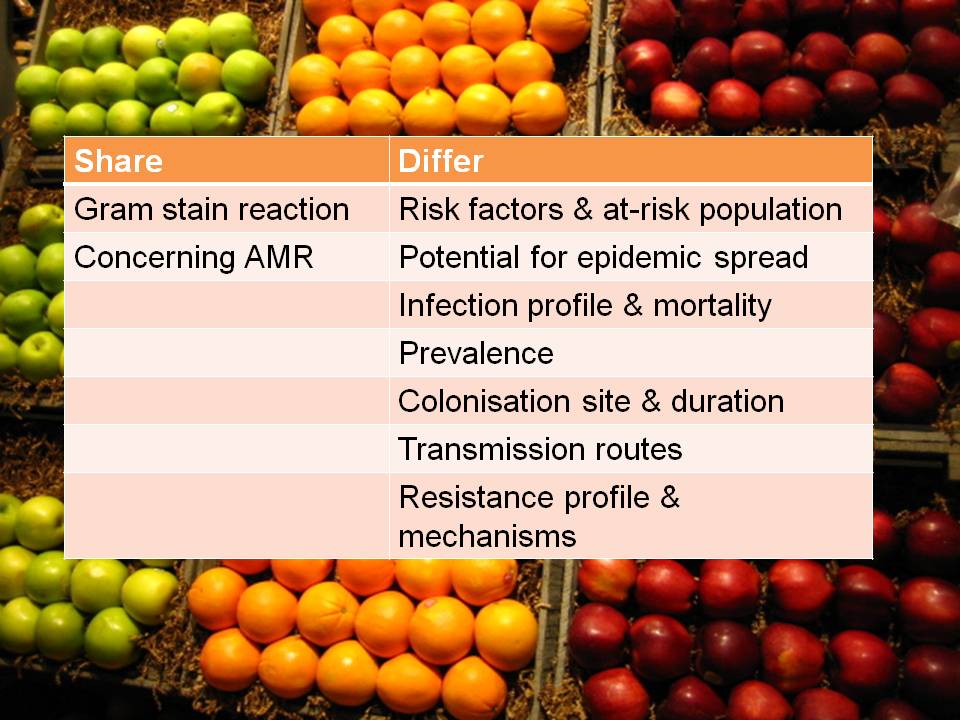
- These resistant organisms inactivate commonly used antibiotics. For any infected patient there are Few Treatment Options and there will eventually be No Treatment Options.
- They are spread Person to Person by touch, splash or contaminated equipment / environments.
- The resistance mechanisms are spread between different species of bacteria.
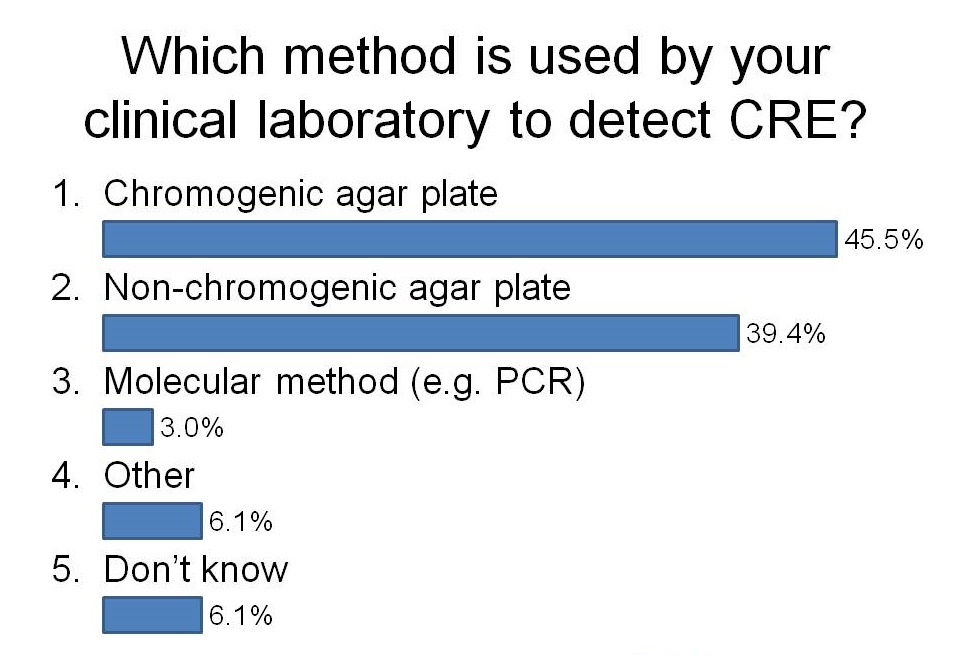
- They are difficult to detect when people are screened.
- They cause outbreaks, which are also difficult to detect and very costly to manage.
- Spread across the world makes at least some transmission here inevitable.
3) Take a ‘high-reliability’ approach to the problem in your area…
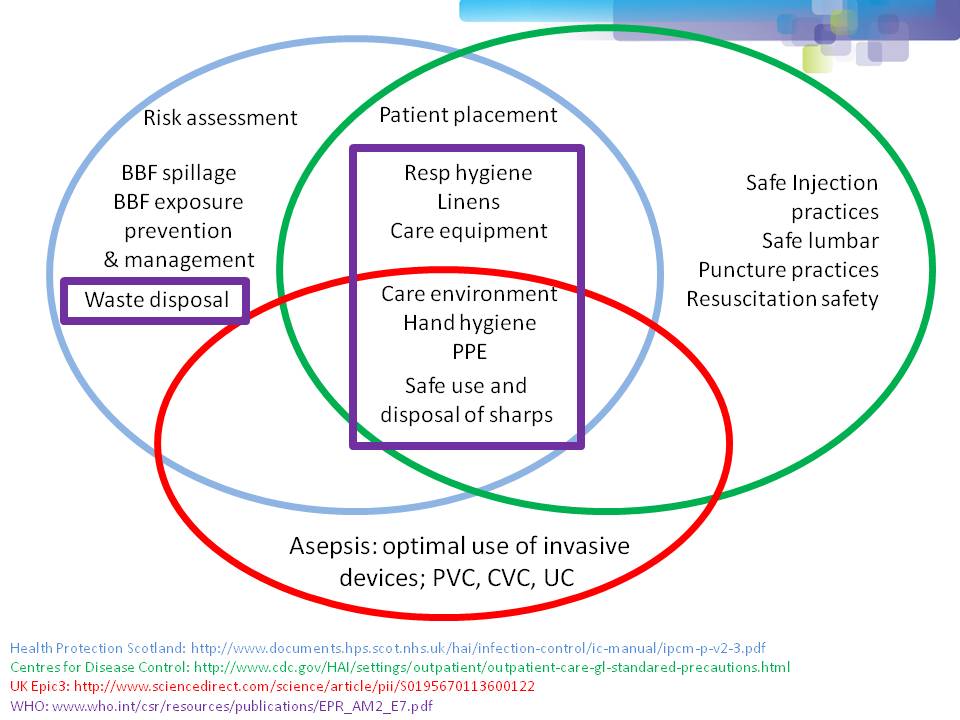
I am not going to regurgitate what is in existing guidelines but offer some high-reliability characteristics.
Sensitivity to operations: Given your patient/client population, consider how and why your healthcare system is vulnerable; share this information within your organisation.
Deference to expertise: Identify who you would go to for expert advice within and outwith your organisation should an incident arise. Keep contact details accessible.
Preoccupation with failure: Consider in which clinical areas you most likely to have an outbreak – visit these clinical areas and see if there can be changes to ways of working that would make outbreaks less likely.
Reluctance to simplify: Look for and don’t dismiss alert signals – this could be data that suggests you may have cases, cross-transmission, that you are insufficiently looking for possible cases or that your antibiotic prescribing data could make your healthcare system more vulnerable.
Commitment to resilience: Good as you and your team are – consider how you can make your systems better at preparedness, prevention and management of outbreaks.
High-reliability theory provides a framework to achieve mindfulness. Google ‘High-Reliability Theory’ and ‘Weick’ for some very useful information.
4) Involve patient advocates
Patient advocates only really knew about MRSA and Clostridium difficile infection when the media told them. Letting patient advocates know that your team is alert to this emerging threat and that you are taking actions to prevent outbreaks may help. They can also lobby for leaders to take further action if required.
Here ends my first blog! Happy I think to receive comment, suggestions or improvements. Thanks for reading. Of note: Outbreak column 17 is on Cognitive Errors in Outbreak Prevention, Preparedness and Management.
Dr Evonne Curran bio:

Evonne is a practicing infection control nurse (since 1987) and a Doctor of Nursing (since 2010). She is the editor of the Outbreak column in the Journal of Infection Prevention (since 2011).















{kind=link}