We have just published an evaluation of Omicron COVID-19 harm as a research letter in the Journal of Infection. This multicentre study reported the findings of a retrospective review of 129 patients with healthcare-associated Omicron COVID-19, and found that the harm profile was very different to previous waves: a small proportion of patients required supplemental oxygen, escalation to critical care, had an extended length of stay, or died from COVID-19. This informs our winter IPC strategy: whilst COVID-19 is more than “just a cold”, the balance between direct and indirect harms from COVID-19 has shifted towards preventing indirect harms (like reduced hospital throughput and delayed diagnosis) and more of a focus on other issues (e.g. flu, Gram-negative BSIs etc).
Continue readingHCAI
Do stand-alone air disinfection units reduce HCAI?
Wow, it’s been ages since I’ve posted – sorry about that. I’m blaming the Omicron wave and my own personal dose of COVID-19 recently (you can see my reflections about that on Twitter…)
And so to today’s blog. Lots of interest in air disinfection systems. And some important research articles coming through. This one in JHI caught my attention, because there’s a suggestion of a link between improved air hygiene and reduced HCAI. However, I am unconvinced (from this study) that this link has been demonstrated – so a key opportunity for applied research!
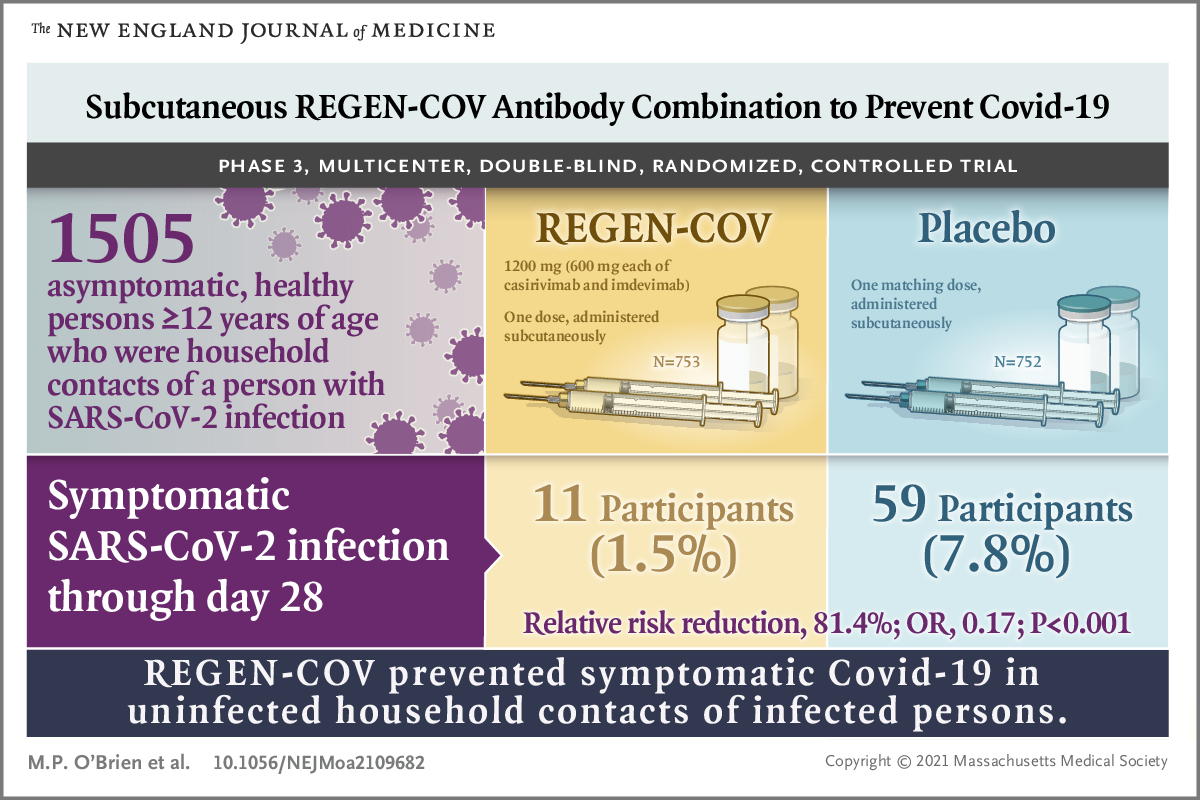
Continue readingMonoclonal antibodies to prevent household transmission of SARS-CoV-2
A remarkable new NEJM study has shown that the prophylactic administration of monoclonal antibodies reduces the risk of household contacts developing symptomatic or asymptomatic infection with SARS-CoV-2. For those who did develop symptomatic infection, monoclonal antibodies reduced to duration of disease and the duration of high viral load. This study opens up the possibility of a new tool to prevent the spread of SARS-CoV-2 to vulnerable patients in our hospitals. Is the future of managing hospital contacts of SARS-CoV-2 the prophylactic administration of monoclonal antibodies?
Antimicrobial copper surfaces and linen and healthcare-associated infection: a review and meta-analysis
A helpful new review and meta-analysis asks whether treating hard surfaces or linen reduces healthcare-associated infections. The review identified only a small number of studies that had both a copper-related intervention related to surfaces and/or linen and an outcome related to HCAI. But the meta-analysis of the seven studies found that, overall, the risk of HCAI was reduced by 27% (risk ratio 0.73, 95% confidence interval 0.57–0.94).
Continue readingThere’s more to IPC & AMS than COVID-19
As parts of the world begin to contemplate life on the other side of this pandemic, it’s time to address that niggle in the back of our minds as our attention has been focussed on COVID-19: what’s been happening with those other HCAI and AMR issues that usually occupy our days (and nights)? This helpful opinion piece in ICHE discusses the impact of COVID-19 on our usual HCAI & AMR practice.
Are the robots taking over? The role of machine learning and AI in tackling infectious diseases

I attended a brilliant seminar at Imperial College last week on the role of machine learning and artificial intelligence (AI) in infectious management, and to a lesser extent, infection prevention and control. There’s so much potential for this exciting technology to revolutionise the way we identify, treat, and prevent the spread of infectious diseases. But, there’s also some risks – some are already asking whether the robots are taking over, and whether that is an entirely good thing!
Infectious disease epidemiology 101
I participated in Imperial College London’s school outreach programme by doing an intro to infectious disease epidemiology with a group of year 10-12 students (age 15-18) (you can download my slides here). It was hugely rewarding and highly recommended for anybody considering supporting this sort of work. The group were sharp, good fun, and asked good questions – and perhaps included one of the next generation of infectious disease epidemiologists?
AMR strategy in the UK: IPC is high on the agenda (hooray)
The Department of Health have published a new 5 year National Action Plan to combat AMR (2019-2024) to follow on from the 2013-2018 edition. IPC and antimicrobial stewardship are high on the agenda – but we have a long way to go if we are to fulfil the 20 year vision for AMR: ‘By 2040, our vision is of a world in which antimicrobial resistance is effectively contained, controlled and mitigated.’
Keeping hospitals clean and safe without breaking the bank

A paper has just been published in ARIC as the first academic output of the Healthcare Cleaning Forum. I blogged earlier this year to relate the inaugural Healthcare Cleaning forum, and this paper expands on the key themes: establishing environmental hygiene as a patient safety initiative, providing an overview of the importance of environmental hygiene in healthcare, exploring the human factors driving the standards of environmental hygiene along with the need for effective education, the possibilities and challenges of automation, and the cost and value of environmental hygiene.
One of the key aims of the forum is to be a champion for environmental hygiene professionals. There’s a famous story of when president JFK visited NASA and asked a janitor who was mopping the floor what they were doing. The answer was simple and profound: “I’m helping to put a man on the moon.” If you asked somebody working in environmental hygiene in your hospital what they were doing, would the response be: “I’m helping to maximise patient safety and prevent healthcare-associated infection.” Probably not. We need to champion the cause of environmental hygiene professionals, who lack professional status, are often not paid enough, and often have limited options for career progression.
Is environmental a treasured investment priority in hospitals?

Related to this is our perception of the cost and value of environmental hygiene in hospitals. Is our level of investment appropriate given the risks associated with inadequate environmental hygiene in hospitals? Would we really find highly valued cleaning and disinfection materials in the metaphorical safe of a hospital manager (see the cartoon above)? Probably not! We need work towards better evidence to understand the value of environmental hygiene in hospitals in the context of other investment priorities.
Nine decades of antibiotics: a story with two endings…
I did a talk today in Portugal covering the nine decades since Fleming discovered the effects of Penicillium sp. in 1928. I thought it would be interesting to have two endings to the talk: an upbeat one, and a doomsday one.
