As parts of the world begin to contemplate life on the other side of this pandemic, it’s time to address that niggle in the back of our minds as our attention has been focussed on COVID-19: what’s been happening with those other HCAI and AMR issues that usually occupy our days (and nights)? This helpful opinion piece in ICHE discusses the impact of COVID-19 on our usual HCAI & AMR practice.
An informal Twitter poll suggested that about 80% of people working in IPC and hospital epi have been spending at least 75% of their professional lives on COVID-19 management. I guess this depends where you are on the curve, but this seems a bit light to me! It’s also worth bearing in mind that the real IPC work begins after the peak of the epidemic when we return to hospitals with a mixture of SARS-CoV-2 infected and SARS-CoV-2 susceptible individuals.
The article outlines how surveillance systems have been interrupted, data collection has ceased, and, due to operational limitations related to single room capacity, staffing, and (in some places) PPE availability, we have managed our “usual suspects” (CPE, MRSA, VRE, C. difficile etc) in a different way (see Figure 1). Antimicrobial stewardship activities have been badly affected, with those working in AMS being diverted to COVID-19 management whilst at the same time, expansion of critical care services, and the prospect of secondary bacterial infection creating an unprecedented demand for optimal AMS activities.
Figure 1: The potential impact of COVID-19 on IPC & AMS activities.
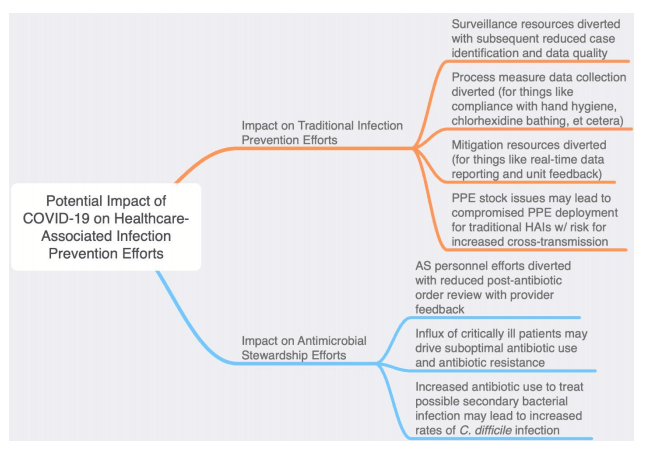
The outcome of these challenges is difficult to predict, but it seems likely that we will see a global increase in HCAI and AMR related to the diversion of resources to the management of the COVID-19 pandemic.
It’s not all doom and gloom though – during this pandemic we have learnt a lot about the value of IPC & AMS, the need for preparation and investment in IPC & AMS services, the importance of routinely collected data for ongoing surveillance, and the ability to rapidly flex the provision of IPC & AMS expertise to meeting emerging needs.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

Hi Jon, What the figure doesn’t mention, though, is that thanks to COVID-19 the bogus hand hygiene compliance of the past have now become a reality! Our CRE incidence has never been better thanks to lower patient numbers (we never bought into the herd immunity theory so have managed to control admission pressures) and massively increased hand hygiene; since everyone is scared senseless about contaminated hands and AHR consumption has sky rocketed.
I guess there is always a silver lining….
Michael
LikeLike