A remarkable new NEJM study has shown that the prophylactic administration of monoclonal antibodies reduces the risk of household contacts developing symptomatic or asymptomatic infection with SARS-CoV-2. For those who did develop symptomatic infection, monoclonal antibodies reduced to duration of disease and the duration of high viral load. This study opens up the possibility of a new tool to prevent the spread of SARS-CoV-2 to vulnerable patients in our hospitals. Is the future of managing hospital contacts of SARS-CoV-2 the prophylactic administration of monoclonal antibodies?
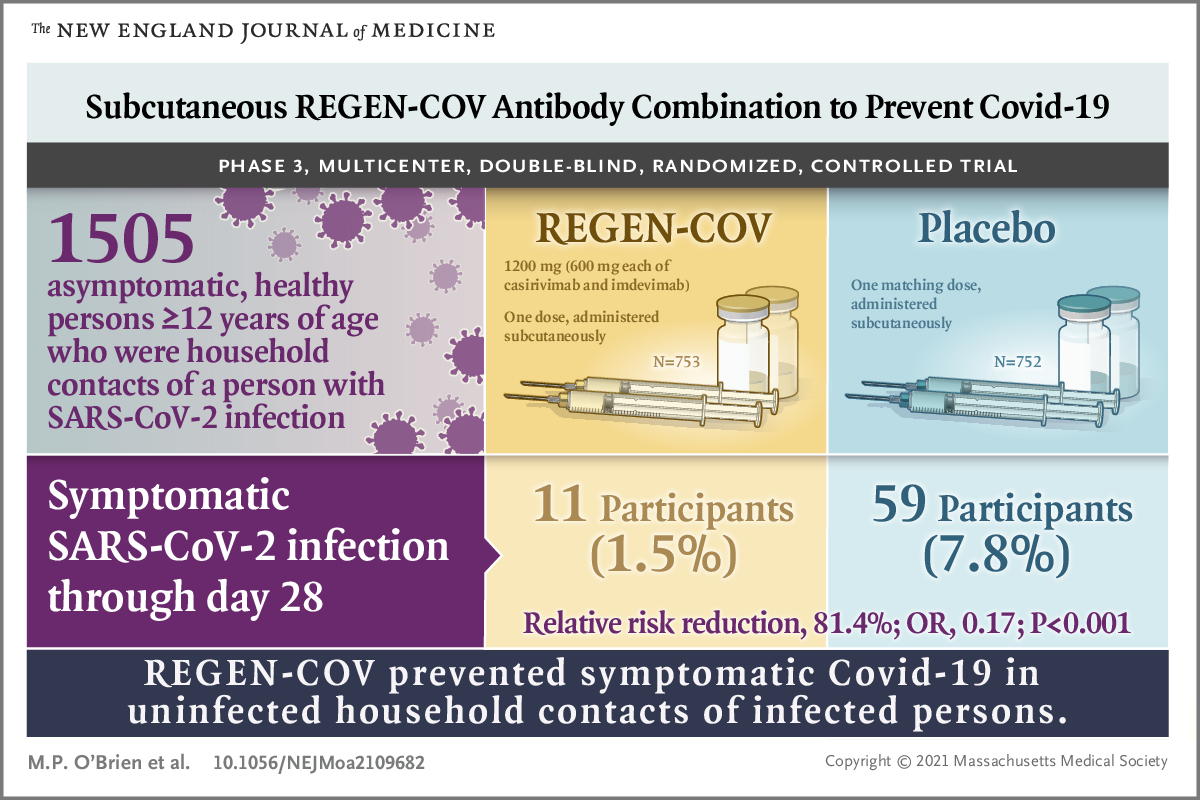
The randomised controlled trial evaluated the impact of REGEN-COV (casirivimab and imdevimab) vs. placebo in preventing household transmission of SARS-CoV-2 following a positive test in the household. A total of 1505 participants were randomised 1:1 to each arm of the study, which was conducted on 112 sites in the USA, Romania, and Moldova. The study included adolescents (12-17 years) and adults (>17 years). Participants were enrolled within 96 hours of collection of the positive test from the index case in the household. Prior to randomisation, a PCR and blood test were undertaken to rule out asymptomatic infection and recent previous infection.
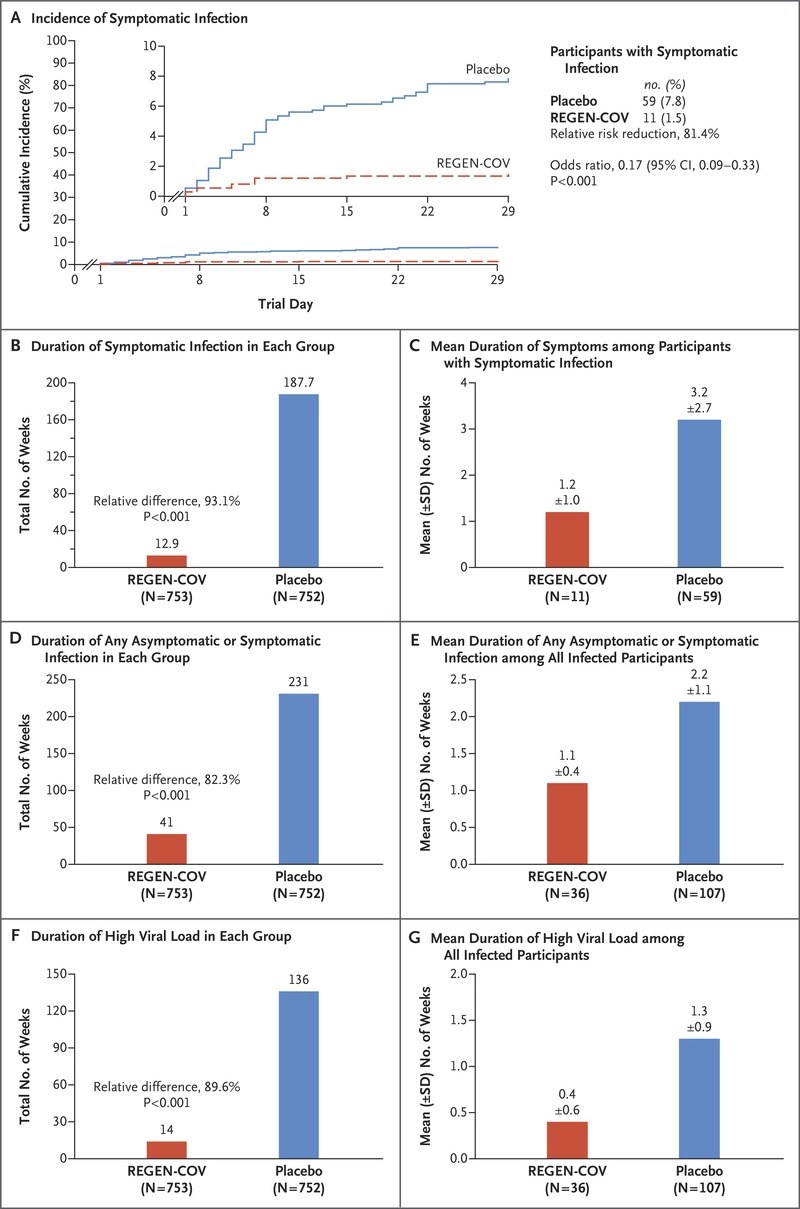
The results were nothing short of spectacular (see visual abstract and the Figure). Monoclonal antibodies dramatically reduced the rate of symptomatic infection (11 of 753 participants in the REGEN-COV group (1.5%) vs. 59 of 752 participants in the placebo group (7.8%) (relative risk reduction, 81.4%; odds ratio, 0.17; P<0.001), asymptomatic infection (36 of 753 participants in the REGEN-COV group (4.8%) vs. 107 of 752 participants in the placebo group (14.2%) (relative risk reduction, 66.4%; odds ratio, 0.31; P<0.001). Monoclonal antibodies also reduced the mean duration of infection (1.2 weeks in the REGEN-COV group vs. 2.2. weeks in placebo), and the mean duration of high viral load (0.4 weeks in the REGEN-COV group vs. 1.3 weeks in placebo). There was no increase in adverse events reported in the REGEN-COV arm – in fact, more adverse events were reported in the placebo arm.
The household attack rate overall in this study was about 25%, which is in line with other studies. And may be a little lower than you’d expect to see. Remember, prolonged close contact is the best way to spread SARS-CoV-2 – it doesn’t spread as effectively as some other viruses. In this study, monoclonal antibodies dramatically reduced the household attack rate. And improved clinical outcomes for those who did get infected. So, the obvious question is should we be administering monoclonal antibodies to all COVID-19 contacts? Well, if we could, then we probably would. But monoclonal antibodies are not widely available yet, so there’s a focus on using them to treat and attenuate symptomatic infection first, then to prevent the progression of disease from mild to severe, and only then to look at using them for prophylaxis.
It’s also important to consider the role of vaccination in all of this. You’d expect the impact of monoclonal antibodies to be less in a vaccinated individual, but also that the effect would increase as the benefits of the vaccine wanes over time.
Can I see a future where all hospital contacts of COVID-19 get a shot of monoclonal antibodies? Perhaps, but I suspect it will be a bit more nuanced than that, involving an assessment of immune status and risk of poor clinical outcome should COVID-19 develop.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
