A rather beautiful review and meta-analysis by colleagues at Imperial College London examines the evidence around the secondary attack rate (SAR) for SARS-CoV-2 in various settings, highlighting the risk of prolonged contact in homes as the highest risk for transmission.
Online databases were searched up to early July 2020 – so a few more articles will have been published since this work was done. Studies included in the meta-analysis reported on setting; the number of index, case-contacts, and secondary cases; tested all contacts regardless of symptoms; and reported on more than one index case. A total of 45 reports were included in the meta-analysis.
The key findings of the meta-analysis are summarised in Table 1. The key point is that household settings had by far the highest SAR – although this was lower than you might expect at 21%. The data for ‘healthcare’ comes from 10 studies – in six of these studies, index cases were all patients, in two studies index cases were both patients and healthcare workers, and in one study, index cases were healthcare workers only. The final study didn’t include this (rather important) info.
Table 1: Pooled SAR for SAR-CoV-2 transmission in various settings.
| Setting | Pooled SAR | 95% Confidence Interval |
| Households | 21.1% | 17.4% – 24.8% |
| Social gatherings with family and friends | 5.9% | 3.8% – 8.1% |
| Travel | 5.0% | 0.3% – 9.8% |
| Healthcare | 3.6% | 1.0% – 6.9% |
| Workplace | 1.9% | 0.0% – 3.9% |
| Casual close contacts | 1.2% | 0.3% – 2.1% |
The review also identified an age effect – transmission to and from those under the age of 20 years was lower (Figure 1).

There’s also a clear and stepwise association between the transmission risk from those without symptoms, in the pre-symptomatic period, and those with symptoms (Figure 2).
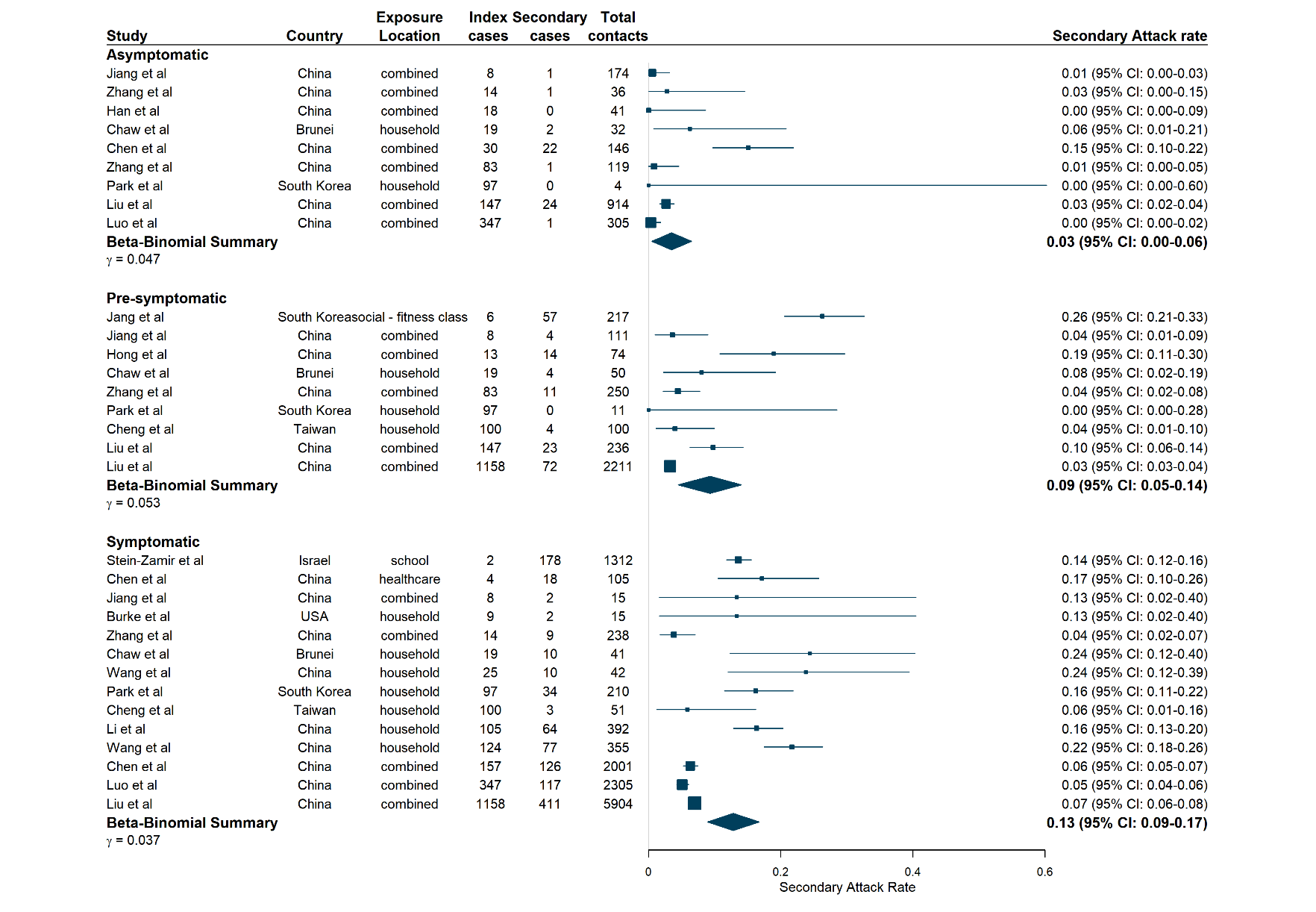
It’s a bit surprising that the secondary attack rates are as low as they are for SARS-CoV-2. To think that transmission of SARS-CoV-2 only occurs for around 2 in 10 contacts underlines that SARS-CoV-2 doesn’t spread like wildfire, even with close and prolonged contact indoors with family members. This gives me hope and confidence that we can effectively prevent the spread of SARS-CoV-2 between patients and staff in healthcare settings.
The finding that household settings had the highest SAR by some margin underpins the UK government advice about avoiding meeting indoors, with a much more relaxed approach to meeting outdoors. It also explains why the approach this Christmas has been (very sensibly) tightened to reduce the number of indoor household contacts.
One of the key features of SARS-CoV-2 is the asymptomatic and pre-symptomatic transmission, which seems much less evident with other similar viruses. It will be interesting to see whether the reasons for the apparent increased transmissibility of the new variant is related to extended asymptomatic or pre-symptomatic shedding.
The key messages of this review are that prolonged indoor household contact is the biggest risk for spreading SARS-CoV-2, that younger people seem less susceptible to acquisition and less likely to spread SARS-CoV-2, and reinforcing that asymptomatic and pre-symptomatic transmission is helping to fuel this pandemic.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
