I have thought a lot (probably too much) about the best way to describe the issue of carbapenem resistance in Enterobacteriaceae. I decided ages ago that CRE (a la the CDC) is the way to go as a generic term to describe the problem. But the more I think about it, the more I am coming around to the idea that CPE (a la PHE) is better. And here’s why:
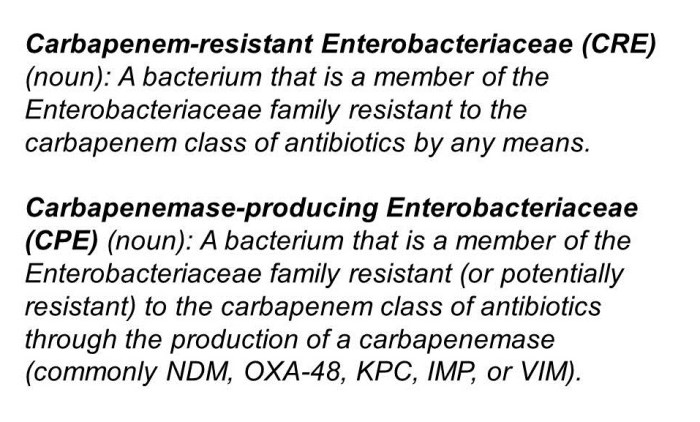
- The real issue from a clinical and infection control viewpoint is CPE. Enterobacteriaceae that are resistant to carbapenems by means other than an acquired carbapenemase (i.e. CRE that are not carbapenemase producers) are important, but they don’t seem to have the same capacity to spread as carbapenemase producers.
- It’s a really confusing situation in terms of terminology. From the “end user” staff member on the front line and patient, all that really counts is whether it is a CPE or not. It’s really rather confusing to tell a patient that the have a “CRE that is also a carbapenemase producer” – easier just to say “you have a CPE”. (I accept that you will also need to tell a patient if they have a CRE that is not a carbapenemase producer – but I think this way around is easier.)
- CPE is already en vogue in the UK (mainly due to the PHE Toolkit) so using any other term risks confusion at the time of patient transfer. (Clearly, this point is reversed if you are working in the US!)
I still think that “CRO/CPO” is not the way to go, given the gulf in epidemiology between the Enterobacteriaceae and the non-fermenters (although, sometimes, begrudgingly, you have to go there). What I mean by this is that you will sometimes detect a carbapenemase gene from a PCR but don’t yet know whether it is from a non-fermenter or Enterobacteriaceae species. In this circumstance, this has to go down as a ‘CPO’.
So, there you have it, a personal U-turn. CRE -> CPE. But I wonder whether CDC and PHE and the international community will ever agree a common term…