The PHE Toolkit recommends pre-emptive isolation for patients who meet one of the risk-factor triggers for CPE screening. Furthermore, the pre-emptive isolation recommended in the Toolkit should be continued until three negative screens are obtained, each separated by 48 hours. In what is best described as a data-based thought experiment, colleagues from Imperial tested the impact of various CPE screening strategies on the burden of contact precautions generated.
Unlike the Toolkit, the study evaluated the contact precautions demand generated by various iterations of screening policies based around universal screening in high-risk specialties, rather than individual risk-factor based screening of all admissions. Benefits of universal screening in high-risk specialties rather than individual risk-factor based screening include ease of administration, potential for a higher impact in reducing transmission, and reduced greater consequence in these high-risk specialties. It’s a shame that the study did not compare the efficacy of universal vs. risk-factor based screening; I suspect that study is for another day…
The study began by ranking the rate of carbapenem resistance in E.coli and K. pneumoniae in various specialties (see Figure 1). This provides a useful model of deciding which specialties are at highest risk for CPE for hospitals who wish to implement universal screening in high-risk specialties.
Figure 1: Rate of resistance to carbapenems in E. coli and K. pneumoniae, grouped by speciality

The contact precautions burden generated by screening all admisisons to the top three specialities (Strategy 1, incluiding the highest risk strategy only; Strategy 2, including the highest and second highest; and Strategy 3, including the top three) were then compared. The proportion of inpatients and potential detection rate of CPE for the 3 screenign strategies is outlined below:
Table: Proportion of inpatients screened and potential CPE detection rate
| % inpatients screened | % CPE detected | |
| Strategy 1 | 4.4% | 17.1% |
| Strategy 2 | 7.6% | 27.8% |
| Strategy 3 | 13.7% | 47.5% |
Strategy 1 = circulation science and renal medicine; Strategy 2 = Strategy 1 + specialist services (including ICUs); Strategy 3 = Strategy 2 + private patients.
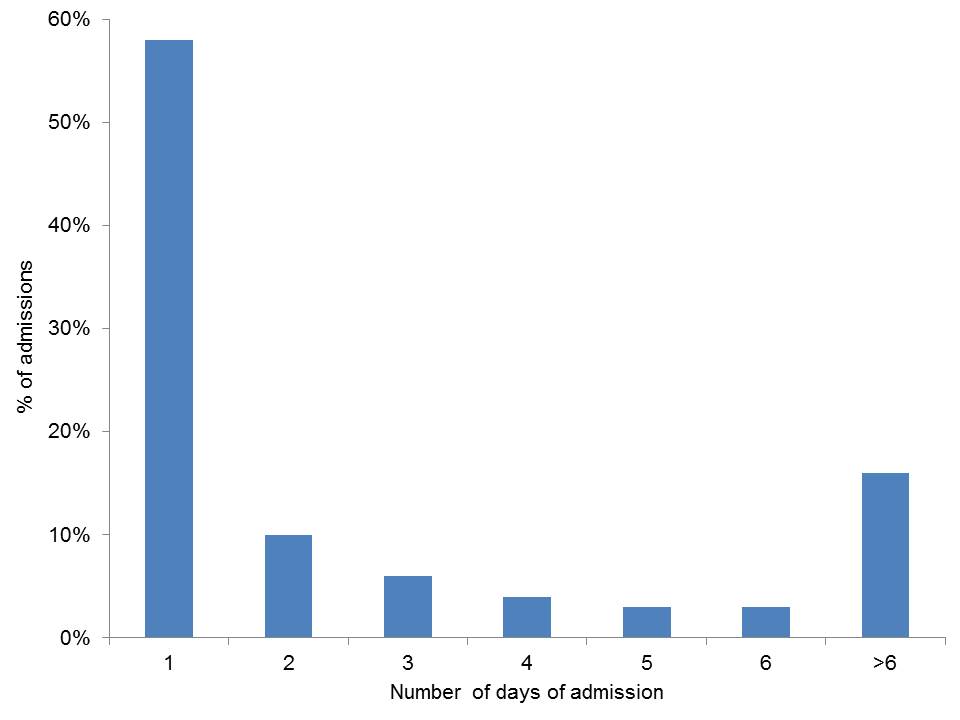
In terms of contact precautions burden generated, the study evaluated 3 scenarios: the first in which only patients with a positive result were put under contact precautions, the second where pre-emptive isolation was applied until the first screen result was available, the third where pre-emptive isolation was applied until the result of 3 screens each separated by 48 hours were obtained. The third scenario here is what the PHE Toolkit recommends. Whether or not pre-emptive isolation was applied made surprisingly little difference to the burden of contact precautions patient days generated – this is because the majority of patients did not stay long enough for their screen result to be available (see Figure 2). However, notwithstanding this point, pre-emptive isolation and waiting for the result of 3 tests would exceed the isolation capacity across the hospital (and by almost 700% in one hospital) so really isn’t feasible. Imagine having ALL of your single rooms filled with patients who are waiting for a CPE screening result!
Figure 2: Number of days hospitalized.
Whilst the purpose of the study was not to compare the efficacy of individual risk-factor based CPE screening with universal screening of high-risk strategies, it is notable that even the most comprehensive screening strategy tested (comprising universal screening of circulation science and renal medicine, critical care, and private patients) would screen 14% of admissions and detect around half of the expected CPE burden. However, put another way, around half of CPE carriers would be missed at the time of admission if universal screening in only these high-risk specialties was performed. Meanwhile, risk-factor based screening of all admissions is likely to result in a considerably higher proportion of admissions being flagged for screening (around 40%), but with an unknown efficacy in detecting carriers. So should we be doing universal screening of high-risk specialties, risk factor based screening of all admissions or a combination of both? The jury is out, but given the potential consequences of failing to detect CPE carriers on admission, we have decided to implement both universal screening in high-risk specialties, and risk factor based screening of all admissions.
Image: Wikipedia.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

{kind=link}