When I started doing research in this area a little over 10 years ago, the role of the environment in transmission was rarely mentioned at international conferences. So, to see an entire conference dedicated to discussing the role of the environment in transmission (SHEA 2013, in Atlanta) was a mouthwatering prospect.
![]()
I’d like to congratulate the organizing committee for putting together such an engaging and entertaining programme. At times, it was true ‘edutainment’. The slides are available here for delegates.
Stephanie Dancer – plenary
The conference began with a plenary lecture by Dr Stephanie Dancer. Irrepressible as ever, Dr Dancer made a good case for improving hospital cleaning (yes, cleaning using detergent and water – not disinfectants). She highlighted some useful older literature, like this paper from 1963 demonstrating that the role of the environment was considered important once upon a time! She also mentioned a useful initiative that she has been involved with in Scotland, mapping visually where contamination occurs in hospital rooms (amongst other things). Dr Dancer finished by covering some of the newer frontiers in the research area, for example resistance plasmids knocking around in the environment, the role of contaminated air in transmission. I enjoyed Dr Dancer’s presentation very much, although contend that detergent and water cleaning is not always enough, now more so than ever as C. difficile and resistant Gram-negatives continue to cause problems around the globe.
Daniel Morgan – fomites
Next up, Dr Daniel Morgan discussed the role of fomites in transmission. I initially thought that this would overlap with the previous and subsequent presentations, but Dr Morgan stuck carefully to his title and considered the role of individual fomites in transmission. Blood pressure cuffs, stethoscopes (or should we say “staphoscope”!), mobile devices and ties (“neck ties” in American English!) were the subject of his reviews. He performed a literature review on each fomite, identifying a surprising amount of literature. I think that contamination of mobile devices is a large and increasing problem, and regular disinfection should be recommended. Dr Morgan also mentioned the interesting looking ‘hospital microbiome’ study in Chicago. Finally, look out for women’s purses (handbags in English English!) as a potential fomite site!
Tara Palmore – water
Waterborne infections were Dr Palmore’s subject. She began by challenging audience perceptions by claiming that all hospitals have had a waterborne infection in the past 12 months. Dr Palmore described an outbreak of Legionnaires’ disease associated with a fountain in a radiology department. Speaking to staff from another hospital after the talk who have had the exact same problem recently makes me wonder how widespread this problem is! The recent problems with Pseudomonas in ICUs in the UK illustrates the potential ramifications of a contaminated water supply. However, we shouldn’t expect sterile water coming out of the taps. If you need sterile water for a patient, use sterile water!
Rekha Murthy – air
Dr Murthy was considering the role of air in the transmission of nosocomial pathogens. She began with a useful classification scheme for pathogens (inspired by this paper) as “obligate”, “preferential” or “opportunistic” in terms of airborne transmission. We know a lot about “obligate” and “preferential” airborne pathogens like TB and ‘flu. It’s the likely “opportunistic” airborne pathogens that are most interesting to me, such as norovirus, MRSA and C. difficile. Sampling indicates that you can find these pathogens in the air, but is contaminated air a vector, and intermediary between the patient and the surface or an innocent bystander?
Curtis Donskey – impact of environmental interventions
Dr Donskey evaluated the evidence that improving environmental disinfection reduces HAIs. He began by drawing a clever parallel between antimicrobial stewardship and environmental hygiene interventions: you can choose to switch product, educate or automate. Dr Donskey demonstrated ample evidence that switching product, educating and automating environmental disinfection has evidence of reducing HAIs. However, he also discussed the potential problem of publication bias, challenging that we don’t like publishing negative findings due to the perception that we’re “admitting defeat”. Publication bias is a real problem in the scientific literature (see, for example, this study showing publication bias in studies of publication bias!). Another potential problem is that, C. difficile aside, almost all studies include the acquisition of colonization rather than the development of infection due to powering issues. This has implications for the cost-benefit of interventions since infections are where most of the cost of MDROs is accrued.
John Boyce – how to culture the environment
Dr Boyce presented everything that you need to know about culturing the environment. He performed a comprehensive literature review and outlined the options: swabs, sponges, enrichment, contact plates, media and other options. My own preferred method is a swab (which can do regular or irregular objects) that is plated direct (to give a quantitative measure of contamination) and then incubated in broth (to give a qualitative but more sensitive measure). With so much heterogeneity in sampling methods, comparison between studies is almost impossible. More standardization in this area would be useful.
Silvia Munoz-Price – measuring cleaning performance
Dr Munoz-Price considered the options for measuring hospital cleaning, presenting her experience with several UV fluorescent markers and ATP bioluminescence. The experience of Dr Munoz-Price is fascinating, finding that the use of environmental cultures along with fluorescent markers was required to drive compliance with cleaning protocols in their ICU. Markers alone lacked credibility (in the eyes of some ICU staff) and cultures alone were not feasible. Also, Dr Munoz-Price’s experience indicates that one fluorescent marking system was better than another since one was more visible under normal light.
David Weber – new technology
Dr Weber covered recent work on some new disinfectant formulations and “no-touch” automated room disinfection (NTD) systems. He presented some impressive data on improved hydrogen peroxide liquid disinfectants, some of which has been published recently by his group. Then, onto NTD systems. Dr Weber began with some useful criteria for adopting NTD systems: firstly they must be demonstrably safe, secondly they must reduce bioburden, thirdly they must reduce infections and finally they must be cost-beneficial. Dr Weber considered the evidence for the four principle NTD options currently available: hydrogen peroxide vapour (HPV) or hydrogen peroxide aerosol, UVC and pulsed-xenon UV (PX-UV). There’s evidence of safety and bioburden reduction for all systems, and evidence of reduced infections (and/or colonization) for HPV. No cost-effectiveness studies published as yet. So, which NTD system to choose? All systems have their pros and cons, so it will depend on your objectives outlined in this recent review, cited by Dr Weber.
James Steinberg and Craig Zimring – the built environment
Engineering solutions to make the hospital environment more amenable to cleaning and disinfection are an attractive option. With a little planning and thought, new hospitals can be built with infection prevention and control in mind at no (or minimal) additional cost. Also, altering the built environment in existing facilities can yield infection prevention and control benefits. Unfortunately, I missed this lecture, but I suspect the content was similar to their recent review article in the ICHE special edition.
Hilary Humphreys – antimicrobial surfaces
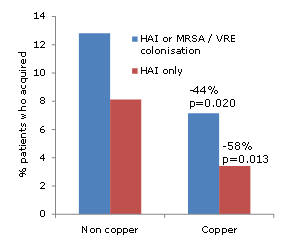
Prof Humphreys gave an accessible overview of the various options to implement antimicrobial surfaces in hospitals. There are various options to consider: metals (principally copper and silver), chemicals or physical changes to surfaces to reduce microbial deposition and/or make them more cleanable. Prof Humphreys mentioned a European testing standard for antimicrobial surfaces that is currently in development and will supersede some (rather wacky) standards that are currently out there. Another problem is that many of the studies supporting the use of antimicrobial surfaces are in engineering journals that seem to speak a different language to the medical literature. Prof Humphreys’ talk helped in interpreting these studies, but more are required in the medical literature. The recently published copper study provides some compelling reasons to prioritize antimicrobial surfaces for further evaluation.
Bill Rutala – disinfectants and microfiber
Dr Rutala presented a convincing case that we should use disinfectants routinely, not just detergents. The main arguments for using disinfectants over detergents for ‘non-critical’ surfaces is that they are more effective at reducing contamination and may have persistent activity, and detergents can become contaminated and spread microbes. It seems that microfiber cloths are better than cotton cloths at removing microbes, but they do harbor them for longer if not disinfected appropriately. So, the evidence for the use of microfiber is somewhat equivocal.
Susan Huang – chlorhexidine bathing
Dr Huang presented three compelling randomized controlled studies evaluating chlorhexidine (CHX) bathing published recently in Lancet, New England Journal of Medicine and one of hers this is not yet published (but doubtless destined for a high-impact journal). The studies seem clear: the introduction of CHX daily patient bathing results in less acquisition, less hand contamination and less environmental contamination. I left the lecture thinking why would you not do this? The potential for reduced susceptibility to CHX is probably the only thing that will stop daily patient bathing using CHX rapidly becoming the standard of care.
Thorny issue #1 – best paths to improve the thoroughness of cleaning (Anne Matlow, Mark Rupp, Larry Nation)
Dr Matlow presented some useful social science exploring the motivations and barriers to compliance with cleaning protocols. Educational deficiencies were identified, for example, almost 40% of housekeepers didn’t think the environment harbored germs that can cause disease. Motivations were explored and it seems that achievement and recognition are more important than pay and advancement.
Dr Rupp presented on the successes and challenges of using audit and feedback to improve compliance with cleaning protocols. Dramatic gains are possible, but it is difficult to sustain the gain. Dr Rupp identified some “positive outliers” during the course of this research. Some would term this group “positive deviants”, but Dr Rupp rightly points out the connotations of this phase are all wrong! There is a potential that these “positive outliers” (if judged by fluorescent markers) are the ones who have clocked the location of the marks and simply spot clean them. Exploring this group in detail will help to confirm that they really are the effective cleaners, and, if so, learn what sets them apart.
Larry Nation is a practicing environmental services director, so was able to provide a complimentary view. His team have moved from visual assessment of cleaning efficacy to a combination of fluorescent marking, ATP and visual assessment to measure the cleaning process and its impact.
All presenters agreed that audit and feedback are essential in setting a path toward improving the thoroughness of cleaning, so Thorny Issue #1 was not all that spiky!
Thorny issue #2 – resistance to disinfectants – Wilcox v Harbarth
Dr Wilcox presented the pro case. Biocide use is gargantuan compared with antibiotic use. However, there is a lot of fear and not much data surrounding biocide resistance. Serial passage of microbes to sub-lethal doses of biocides can induce tolerance, and triclosan is most susceptible to resistance. An area with much equivocal data is the possibility of resistance or reduced susceptibly to skin antiseptics such as CHX. The widespread and most likely increasing use of CHX means that reduced susceptibility would be problematic to say the least. Dr Wilcox presented some compelling data (including some from Dr Harbarth!) that reduced susceptibility to CHX is a problem.
Dr Harbarth presented the con case, although conceded that resistance to skin antiseptics could be a major problem in the future. Dr Harbath argued that antiseptics are a major part of the solution to controlling resistant micro-organisms, not driving the development of the problem! There is very limited evidence of the interaction between antibiotic and biocide resistance and evidence of small reductions in susceptibility that are well below the in-use concentration are not relevant.
On balance, an entertaining debate, and both speakers agree that reduced susceptibility to skin antiseptics is the most likely risk. There is some evidence that small reductions in CHX susceptibility may be relevant even when well below in-use concentrations, and that this may have implications for antibiotic cross-resistance (buried deep in Table 4 of Vali et al. 2008 – look what happened to EMRSA-16 after 48 hours sub-lethal exposure to CHX).
Thorny issue #3 – sporicides for C. difficile – McDonald v Dubberke
Dr McDonald took the pro position, and presented the evidence underpinning the CDC recommendation to use an EPA-registered sporicide for disinfection of rooms potentially contaminated with C. difficile spores. Whilst removal of spores (rather than chemical inactivation) is an important part of the disinfection process, the use of sporicidal disinfectants prevents the dispersal of spores around the room on contaminated cloths. Overall, the evidence for the use of a sporicide to control the spread of C. difficile is overwhelming.
Dr Dubberke presented a rather unenviable con position, given the volume of data supporting the use of a sporicide. However, he did put together a coherent case, highlighting the academic limitations of studies supporting the use of a sporicide, reiterating the risk of publication bias and that practice is more important than product.
Both authors agree that introducing a sporicide will not solve your C. difficile problems; you need to consider all aspects of transmission for that (antimicrobial stewardship, patient susceptibility factors and others). However, the con case presented by Dr Dubberke was not persuasive enough to convince me to abandon the use of a sporicide to help control C. difficile.
Thorny issue #4 – hands v environment – Edmond v Anderson
This debate has been run at several recent conferences so I was concerned that it would be a little “old hat”. How wrong I was.
Dr Boyce (who was chairing) polled the audience at the start of the debate, finding that around 90% thought that hand hygiene is more important than environmental disinfection in preventing HAIs.
Dr Edmond began with the pro. He began by a “thought experiment”, showing that a cluster RCT to compare the impact of the two interventions is not feasible. Dr Edmond acknowledged that there is more and better evidence for environmental interventions than for hand hygiene, but argued that hand hygiene makes a larger contribution to prevention and control. He evaluated the prior room occupancy studies and concluded that the increased risk from the prior occupant only accounts for a small minority of all transmissions.
Dr Anderson’s presentation for the con was outstanding; full of thoughtful, well-constructed arguments. He began with some quotes including the classic “I got 99 problems but the [bleach] ain’t one”; I suspect it was lost on a fair proportion of the audience, but a highlight of the conference for me! Dr Anderson’s argument focused on the fact that there is more and higher quality evidence for environmental interventions than for increased hand hygiene, having scoured the lengthy hand hygiene guidance documents to find a small handful of high-quality studies. In contrast, there are now a number of high-quality studies demonstrating the impact of environmental interventions.
The post-debate vote indicated a swing towards the importance of environmental disinfection, but still the majority concluding that hand hygiene is most important. There can be little doubt that hand hygiene prior to patient contact is the single most important intervention to prevent the spread of hospital pathogens, but it seems that the contribution of the contaminated environment is considerably greater than we thought.
Some points for discussion currently on my mind, mainly prompted by meeting:
- Should we have a standardized set of environmental sites to sample and a standardized way to sample them to make studies more comparable? (A suggestion by Prof Hilary Humphreys.) I like this idea very much. The only problem is that it may result in widespread “targeting” of these sites only by housekeepers!
- “The ward is very big; your swab is very small” (Dr Dancer). Are we sampling a large enough surface area? The CDC sponge method will help with this.
- Can the introduction of single rooms in multi-occupancy bays contain pathogens more effectively (prompted by this image from Dr Weber)?
- What is the contribution of contaminated air in “opportunistic” airborne pathogens (such as norovirus, MRSA and C. difficile)?
- How much of a problem is publication bias? Do we really all have negative environment studies that we have not got around to publishing as suggested by Dr Donskey?
- When are NTD systems warranted, and which NTD system is suitable for the intended application?
- Should CHX ‘source control’ be implemented universally across the hospital?
- Are antimicrobial surfaces going to be useful in preventing transmission, and, if so, which is the most effective?







{kind=link}