You may think so, with this title: “Oral mucositis as a pathway for fatal outcome among critically ill patients exposed to chlorhexidine (CHX)”, with the conclusion that the “data points to oral mucositis as the main pathway for the association between CHX exposure and enhanced in-hospital mortality.” The research letter is a post hoc analysis of a randomized clinical trial. Time to stop using CHX mouthwash? Or time to stop building strong stories on weak data? Continue reading
Ethnicity and infection: avoiding spurious associations
I’ve been meaning to blog on this editorial about ethnicity as a risk factor (or not!) for infection by Prof Leibovici in Clinical Microbiology and Infection for a while. The basic story is that “ethnicity” often falls out as associated with infection-related variables (e.g. colonisation or infection with resistant bacteria), but the editorial poses an important question: it is actually ethnicity, or something co-correlated with ethnicity (e.g. socio-economic status) that is the causal risk factor?
On the origin of multidrug-resistant Gram-negative bacteria (MDR-GNB)
The colour of the global crisis of antibiotic resistance is red (if te Gram stain is your reference). In rich countries we have ESBL-producing Enterobacterales (mainly E. coli), but the real problem are carbapenemase-producing strains (Klebsiella, Pseudomonas and Acinetobacter) that are already endemic in lower and middle-income countries. The unanswered question is “where did these resistant bacteria come from”? Animals or bathrooms? Continue reading
ESPAUR 2019: a snazzy facelift
The 2019 edition of the ESPAUR report has recently been published, including data up to and including 2018. The report is an excellent read – here’s a few summary points.
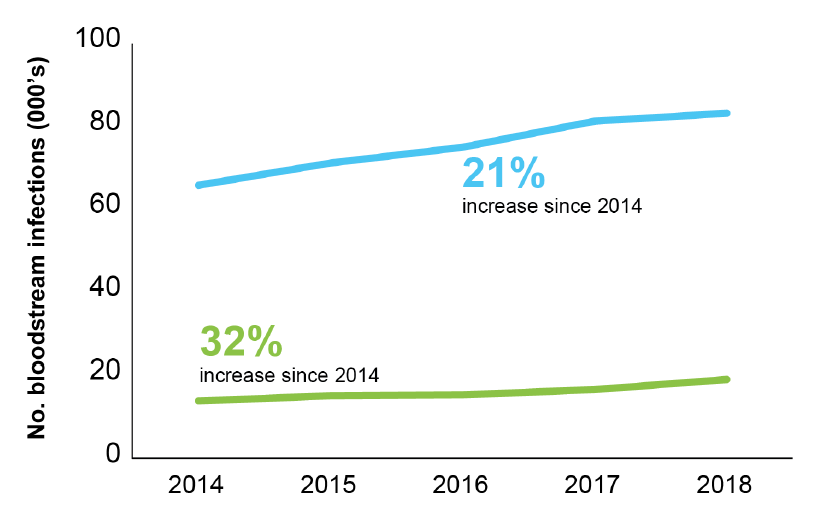
- There’s a series of lovely infographics at the start of the report. I gave myself a challenge: to select the one infographic that told the story of the report. I toyed with the one about a small but increasing number of CPE BSIs (aghhhhh!), and the stark grave-stone themed image of mortality related to carbapenemase-producers, but ended up with this one: alarmingly, the rate of BSI for the seven priority bacterial pathogens rose 22% between 2014 and 2018 to 145 per 100,000 population. (Around half of these were coli). And there’s a certain inexorability about the antimicrobial resistance trends included in this report, with a 32% increase in AMR BSIs comparing 2014 to 2018.
Figure: Trends in BSIs (blue line) and AMR BSIs (green line).
- There were more than 60k antibiotic resistant severe infections in 2018, <150 per day.
- Confirmed CPEs have topped 4k (but this is a gross underestimate of true prevalence). The report makes the case that the rarity of CPE BSIs (142 reported nationally) represents a success of prevention. This is probably true if we compare across the pond and towards the southern reaches of Europe. But difficult to be sure without a control (i.e. what would have happened without the national initiatives etc)? Also, reporting of CPE BSIs to PHE is voluntary and not mandatory, so there will be some degree of under-reporting.
- Related to this, only 50% of diagnostic labs have introduced methods to detect CPE locally. Which links closely with the change in surveillance system for CPEs going forwards – rather than manual voluntary reporting, locally confirmed CPEs will be reported automatically to PHE. However, if only 50% of diagnostic labs have appropriate methods, we’ll still end up under-reporting (but it will be more a more accurate picture than the current process provides).
- 30 day all-cause mortality of invasive CPE infections is 24% (along with the arresting gravestone-themed infographic)! Not sure how helpful it is to make a big point based on unadjusted mortality data…
- Overall consumption of antibiotics continues to decline. Consumption fell from 20 to 18 DDDs per 1,000 population per day between 2014 and 2018. However, consumption increased by 3% in hospitals over this period.
- There’s a nice section on Candida auris
- ESPAUR reports some good work and outcomes related to training, education, and awareness (e.g. Keep Antibiotics Working and Antibiotic Guardian).
- What a wonderful resource the AMR Fingertips module is: automated data from >90% of NHS laboratories on a range of AMR indicators at our…ahem…fingertips. I am one of the 15k users over the past three years. (As an aside, the volume of traffic is fairly low by popular website standards – but I guess it is somewhat niche!)
ESPAUR is a fantastic resource – it seems that this is the last ESPAUR report related to the UK AMR Strategy from 2013-2018, but I’m confident that ESPAUR will continue to report the successes and challenges of implementing the new five year action plan (from 2019-2024).
CPE infection prevention and control guidelines: an update
Since writing this 2015 review on gaps and controversies in the guidelines for the prevention and control of CPE (and other MDR-GNR) I’ve tried to keep it fairly up to date. So, here’s the latest iteration, including the 2015 CDC guidelines.
The infinite trio from South Africa
Last week I had the pleasure of attending the 8th FIDSSA Congress in Johannesburg (Federation of Infectious Diseases Societies of Southern Africa). I was invited to talk on infection control in the Netherlands, SDD and empiric antibiotic strategies in ICU. I never felt more distance between my habitat and that of my hosts. It surpassed the 3732 miles in the air. I learned a lot; from how it is to go into military conflict areas to identify Ebola cases, fighting a cholera outbreak after a tropical cyclone in Mozambique to the infinite trio, which stands for carbapenem resistant Klebsiella, Pseudomonas and Acinetobacter. Continue reading
CPE carriage – once positive, always positive…or maybe not?
I blogged recently about the new ESCMID guidelines on resistant Gram-negative carriage and decolonisation, which supported a “once positive, always positive” approach to CPE carriers due to the lack of effective decolonisation options. A new study suggests that a large majority (75%) of patients who were once identified as CPE carriers no longer had CPE detectable when they were readmitted. This has implications for the management of CPE carriers in hospitals.
Single rooms for ESBLs anyone?
A comprehensive and impressive cluster randomised crossover study published in Lancet ID examines whether it makes sense to use single rooms (as compared with multi-bed bays) to apply contact precautions for patients known to be carrying ESBL-Enterobacteriaceae. I need to be careful what I say, because fellow bloggers Marc and Andreas are co-authors. However, the gist seems to be: don’t bother with single rooms for ESBL-E carriers – but many hospitals don’t have capacity to do that anyway, so this may not be a practice-changing finding in many parts of the world!
Formatting scientific papers: a waste of time, money, and grey matter!
Those of you who have published a scientific paper or two will recognise the following process:
Format.
Submit.
Reject.
Reformat.
Submit.
Reject.
Reformat.
Submit.
Accept.
By the end of this process, not only have you lost the will to live (or ever reformat a scientific paper ever again), you’ve also wasted time = money. And chances are, the money has been entrusted to you to perform research, not reformat documents! A recently study counts the cost of this process, concluding that the average scientist spends 52 hours per person per year on formatting / reformatting scientific papers, with a cost of around $500 USD per manuscript or ~$2k per year.
Intra-operative vancomycin: to randomize or not
Today we discussed a recent paper published by our orthopedic surgeons on using powdered vancomycin in the wounds of spinal surgery to prevent surgical site infections (SSI). Two years ago I already had a post on the topic. The powder is spread deep in the wounds, on the bone and metal, before fascia and skin are closed. Yet, none of the 3 guidelines addressing prevention of surgical site infections that appeared recently recommends this intervention; WHO (2016) didn’t even include the intervention, CDC (2017) said “don’t do it”, and NICE (2019) acknowledged that the procedure is widely used without strong supporting evidence and recommended: stop doing it and do a trial. Continue reading
