By Andreas Voss, Jan Kluytmans and Alexander Friedrich
As the surge of COVID-19 cases is hitting some of the Dutch hospitals hard, healthcare, in the areas being overwhelmed with cases, experience a shortage of PPEs and especially masks. In other Dutch regions with no or only a few cases, colleagues still believe that life is normal and PPEs can be ordered with a click on the computer. They look with awe at what colleagues in the midst of battling COVID-19 and shortages are facing. In addition, all healthcare-settings that do not usually use a lot of PPE’s (e.g. nursing homes and GPs), will be heavily understocked.
Still, infection control advice seems to be based on standard, safety-maximized procedures, thereby wasting valuable resources. As a consequence, HCWs in the Netherlands are still following these recommendations, by using FFP masks routinely, in low risk situations, while they should be saved for the high-risk procedures.
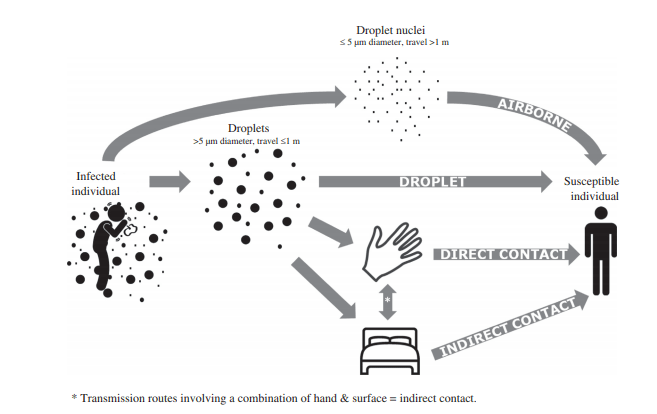
We believe that it is time to rethink our protocols, based on the fact that we still assume that COVID-19, in general, is based on droplet and contact transmission.
- Restricted and risk-based use of FFP masks
- Use of surgical masks for normal care of COVID patients
- Efficient and extended use of FFP masks and other PPEs
- Re-use of FFP masks