The role of surface contamination is increasingly recognised in the transmission of certain nosocomial pathogens1. The most compelling evidence comes from the finding that admission to a room previously occupied by a patient infected or colonised with some multidrug-resistant organisms (MDROs) increases the risk of acquiring that MDRO for the subsequent room occupant by a factor of two or more1-3. Conventional cleaning and disinfection does not reliably remove all environmental MDROs4,5. Hence, it seems that inadequate terminal disinfection of hospital rooms explains the association with the increased risk of acquisition from the prior room occupant. It follows, then, that improvements in terminal disinfection should reduce the levels of residual contamination and the transmission of pathogens through this route. A recent study from Johns Hopkins Hospital tested this hypothesis through the introduction of hydrogen peroxide vapour (HPV) terminal disinfection of selected patient rooms6.
A 30-month prospective cohort intervention study was performed on 6 high-risk units (5 ICUs). HPV was implemented on 3 of the units following a 12-month pre-intervention phase. Clinical impact was assessed by a cohort study. Each patient admitted to any study unit during both phases was included in one of three cohorts:
- ‘MDRO-standard’ Patients admitted to a room where the prior room occupant had an MDRO and the room was disinfected using standard methods.
- ‘MDRO-HPV’Patients admitted to a room where the prior room occupant had an MDRO and the room was decontaminated using HPV
- ‘No MDRO-standard’ Patients admitted to a room where the prior room occupant was not known to have an MDRO and the room was disinfected using standard methods.
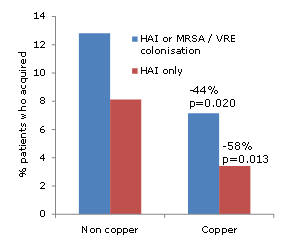
The key finding was that patients admitted to rooms decontaminated using HPV were 64% less likely to acquire any MDRO (incidence rate ratio [IRR] of the MDRO-HPV vs. MDRO-standard cohorts = 0.36, confidence interval CI=0.19-0.70, p<0.001) (see chart below).
Chart showing the MRDO acquisition rate in the three patient cohorts.

‘MDRO-standard’ = Patients admitted to a room where the prior room occupant had an MDRO and the room was disinfected using standard methods. ‘MDRO-HPV’ = Patients admitted to a room where the prior room occupant had an MDRO and the room was decontaminated using HPV.
‘No MDRO-standard’ = Patients admitted to a room where the prior room occupant was not known to have an MDRO and the room was disinfected using standard methods.
The difference between cohorts was adjusted for patient level variables such as length of stay, morbidities and other variables that could explain the difference. This means that the difference between cohorts is attributable to HPV alone. When broken down into individual MDROs, the largest reduction was shown for VRE (a 75% reduction, p<0.0001). HPV provided a protective effect for the other MDROs assessed (C. difficile, MRSA and MDR-Gram-negative rods), but differences for these individual pathogens were not statistically significant.
Surprisingly, even when the prior room occupant was not known to have an MDRO, HPV reduced the risk of acquisition by 51% (comparing the MDRO-HPV with the No MDRO-standard cohort). You’d expect the acquisition rate in the ‘MDRO-HPV’ cohort to match the ‘No MDRO-standard cohort’. In fact, it is lower. This is likely due to survival of contamination from previous occupants, unrecognised colonisation or introduction by healthcare workers.
Environmental impact was assessed by sampling each patient room on all units monthly for the last 3 months of the pre-intervention phase and the first 6 months of the intervention phase. Swabs were collected from all patient rooms, occupied or unoccupied, regardless of patient status. The overall percentage of rooms contaminated with one or more MDRO was reduced significantly when HPV was in operation. Further, rooms contaminated with multiple MDROs, occasions when the MDRO from room differed from the room occupant’s known MDRO and MDROs cultured from empty rooms were less likely when HPV was in operation.These changes are due to improved terminal disinfection using HPV.
Whilst this study is one of the few to evaluate patient outcomes in addition to environmental impact of a no-touch automated room disinfection system7. it does have several limitations, some of which are highlight in an accompanying editorial8. Firstly, the rooms or units were not randomized to an intervention arm, which could have introduced bias. Secondly, whilst the conventional disinfection methods were optimized prior to the introduction of HPV, more could have been done to improve the efficacy of conventional methods which may have over-estimated the impact of HPV. Thirdly, the low prevalence of acquisition (especially for MDROs besides VRE) made detecting changes in incidence difficult. Fourthly, whilst the infection rates in the three cohorts did not change significantly with study phase and the clinical impact on an individual patient level was impressive, overall unit level changes in rates of infection were not reported.
The study has important implications for the proportion of transmission that is likely to involve contaminated surfaces. Extrapolating unadjusted data from the study indicates that 16.7% of the acquisitions that occurred during the study were attributable directly to the prior room occupant. This figure most likely underestimates the total contribution of contaminated surface to nosocomial transmission because contaminated surfaces are likely to be involved indirectly in transmission during the stay of affected patients1.
In summary, HPV disinfection significantly reduced the risk of patients acquiring MDROs from previous room occupants in high-risk settings. Furthermore, HPV also provides a protective effect even when the prior room occupant was not known to be infected or colonised with an MDRO. These clinical findings are supported by environmental data showing that HPV disinfection improves the efficacy of terminal disinfection, thus reducing environmental contamination. Whilst the study is not without its limitations, it takes the question of how to tackle hospital environmental contamination forward a pace or two.
Article citation: Passaretti CL, Otter JA, Reich NG et al. An evaluation of environmental decontamination with hydrogen peroxide vapor for reducing the risk of patient acquisition of multidrug-resistant organisms. Clin Infect Dis 2013; 56: 27-35.
References:
1. Otter JA, Yezli S, French GL. The role played by contaminated surfaces in the transmission of nosocomial pathogens. Infect Control Hosp Epidemiol 2011; 32: 687-699.
2. Drees M, Snydman D, Schmid Cet al. Prior environmental contamination increases the risk of acquisition of vancomycin-resistant enterococci. Clin Infect Dis 2008; 46: 678-685.
3. Huang SS, Datta R, Platt R. Risk of acquiring antibiotic-resistant bacteria from prior room occupants.Arch Intern Med 2006; 166: 1945-1951.
4. Manian FA, Griesenauer S, Senkel Det al. Isolation of Acinetobacter baumannii complex and methicillin-resistant Staphylococcus aureus from hospital rooms following terminal cleaning and disinfection: can we do better? Infect Control Hosp Epidemiol 2011; 32: 667-672.
5. French GL, Otter JA, Shannon KP, Adams NM, Watling D, Parks MJ. Tackling contamination of the hospital environment by methicillin-resistant Staphylococcus aureus (MRSA): a comparison between conventional terminal cleaning and hydrogen peroxide vapour decontamination. J Hosp Infect 2004; 57: 31-37.
6. Passaretti CL, Otter JA, Reich NGet al. An evaluation of environmental decontamination with hydrogen peroxide vapor for reducing the risk of patient acquisition of multidrug-resistant organisms. Clin Infect Dis2013; 56: 27-35.
7. Otter JA, Yezli S, Perl TM, Barbut F, French GL. Is there a role for “no-touch” automated room disinfection systems in infection prevention and control? Submitted. J Hosp Infect 2013; 83: 1-13.
8. McDonald LC, Arduino M. Climbing the evidentiary hierarchy for environmental infection control. Clin Infect Dis 2013; 56: 36-9.