 A little while ago I blogged about the excellent study from Nottingham that demonstrated significant VRE and MRSA contamination on socks used to prevent falls in the hospitalised elderly. This has been followed by another paper suggesting that shoe coverings undurprisingly become contaminated. So, what? How does this really impact on transmission? A new study from Curtis Donskey’s group has looked at hand contamination in patients directly relating to floor contamination. Continue reading
A little while ago I blogged about the excellent study from Nottingham that demonstrated significant VRE and MRSA contamination on socks used to prevent falls in the hospitalised elderly. This has been followed by another paper suggesting that shoe coverings undurprisingly become contaminated. So, what? How does this really impact on transmission? A new study from Curtis Donskey’s group has looked at hand contamination in patients directly relating to floor contamination. Continue reading
transmission
PPE for preventing highly infectious diseases

The use of PPE and the protection of HCWs against highly infectious diseases was (and is) a topic of major importance, around the globe. The recent Cochrane review by Verbeek et al. was probably hoping to offer this “vital” information.
Unfortunately, they found no studies on the effects of goggles, face shields, long-sleeved gloves or taping on the risk of contamination. All they found was very low quality evidence, with high risk of bias and uncertain estimates of effect, that:
- More breathable types of PPE offer more comfort without increasing the risk of contamination
- Double gloving and CDC doffing guidance appear to decrease the risk of contamination, and
- Active more than passive training in PPE use may reduce PPE and doffing errors.
Their conclusions are obvious: we need high-quality studies of the materials, their use and protective effects, safe ways of doffing, and the most adequate training to achieve safe use of PPE for HCWs in the presence of highly infectious diseases or those (even less infectious) that may cause severe harm to HCWs.
But what to do until than? My personal opinion is that we should only use PPE, we are used to and know how to use. First-time users, even if supplied with the best available products, will inevitably fail to remove the PPE without error. Consequently, institutions should have a stable selection of PPE, and in the case of preventing highly infectious diseases, a selected group of HCWs with continuous active training, as it is too late to start when the next epidemic is hitting our healthcare centers.

Probable Person-to-Person Transmission of Legionella
Ana M. Correia and colleagues (N Engl J Med 374;5 February 4, 2016) present a convincing case of person-to-person transmission of Legionnaires’ disease between son and mother. Seen the epidemiology of the two cases and the results of whole-genome sequencing, the only part of the short report I do not understand is the “probable” in the title. I wouldn’t know what else to include in order to call it “proven”.
Consequently, the question is whether this “new” transmission route has implication for infection control in the hospital setting. The mother had very close contact over an extended amount of hours with her severely coughing son, in a small and badly ventilated room. In opposite to HCWs who in this situation generally would wear a mask, she obviously used no personal protective equipment. Finally, while described as formerly healthy, no further details are given about the conditions possibly increasing the susceptibility of the 74-year old to Legionella.
Thus, while person-of-person transmission seems proven in the present case, I believe that the circumstances are unique and don’t require to change the present infection control measures taken in patients with Legionnaires disease.
Community MRSA preys on the poor and deprived

As you can probably tell from the title, this post comes with a warning: it presents some rather “un-PC” data, but I’ll do my best to deliver it calmly and dispassionately! My old research team from KCL have just published a paper in PLOS Medicine on the association between social and material deprivation, and MRSA.
I’ve been interested in the dynamic between hospital-associated (HA) and community-associated (CA) MRSA for years (not least because it was the subject of my PhD thesis). I wrote a review several years ago on how community MRSA should be seen as a genotypic phenomenon with epidemiological implications. Using this framework, it is possible to get your head around CA strains of MRSA beginning to cause hospital-acquired infections. The aim of this study was to use a large collection of MRSA from across several regions of London to explore the transmission dynamics and epidemiological associations of HA and CA types of MRSA.
3.. 2.. 1.. Zero. Great, the 48 hours are up!
 We often see those tasked with finding suitable isolation facilities counting down to when precaustions can be discontinued and the ’48 hours clear’ of symptoms of loose stools or vomiting has almost become one of the most welcome statements heard in healthcare settings. No more contact precautions, no more disinfectants sloshing around, normality beckons.. Or should it? Continue reading
We often see those tasked with finding suitable isolation facilities counting down to when precaustions can be discontinued and the ’48 hours clear’ of symptoms of loose stools or vomiting has almost become one of the most welcome statements heard in healthcare settings. No more contact precautions, no more disinfectants sloshing around, normality beckons.. Or should it? Continue reading
It’s transmission doc, but not as we know it
A groundbreaking study just published in PLOS Genetics provides new insight into the transmission dynamics of bacteria in the ICU setting using WGS. The ambitious authors performed WGS on virtually all bacterial isolates from ICUs in a US hospital for a year. The first surprise was that 12% of the bacteria considered clinically relevant were previously undescribed.
The next – and perhaps biggest – surprise was that whilst transmission of the usual suspect pathogens (MRSA, VRE etc) was rare, 9% of the other bacteria were shared by multiple patients, often with overlapping admissions (see the figure below). This suggests that there is a fair bit of transmission going on under the radar in the ICU setting.
Figure: Clonal lineages extending across multiple patients.

This study reminds me of one published in CID a few years ago showing that outbreaks of resistance probably occur regularly and usually undetected across multiple species.
So, is it time to start using WGS for all bacteria identified in the clinical laboratory? Not quite yet I don’t think: the analytical methods have not yet caught up with the sequencing technology. But this study is a glimpse of the future, no doubt about it.
You wait for ages, and then two come at once..

Sometimes waiting for research highlighting an issue that you know is a problem is like waiting for a bus.. Following on from my colleague @jonotter who last week posted about MRSA spread in nursing home settings, I was interested to read this new paper from the USA, published in the Journal of the American Geriatric Society. The study notes the high prevalence of Multi-Drug Resistant Organism (MDRO) carriage in nursing homes that was in excess of that in hospital settings and sought to determine any associations. The findings are interesting, if not surprising.
CRE winging its way around the world

CRE are known to be adept at hitchhiking around the world, hence the focus on cross-border transmission in Europe. A startling example of this comes in a report from Poland result from the terrorist shootings in Tunisia. Two Polish nationals seriously injured in the shootings were repatriated following a 10-day stay in a hospital in Tunis, Tunisia. A grand total of four CREs were identified from the two patients!
Three of these were identified at the time of admission, so almost certainly originated in Tunisia. The fourth CRE was identified 10 days after repatriation to Poland. The authors suggest that the most likely explanation for this is poor sensitivity of admission screening. I venture, however, that it’s more likely due to in-hospital transmission in Poland, since the two patients were treated by the same staff.
Nonetheless, the most troublesome finding here is that at least three separate CREs were imported into Poland by just two patients. Can anybody find me a paper on the prevalence and epidemiology of CRE in Tunisia? No? Thought not. The implication here is that CRE is already far more established than feared in Tunisia and many other parts of the world!
Image: Aeroplane.
Which transmission route is most important for influenza?
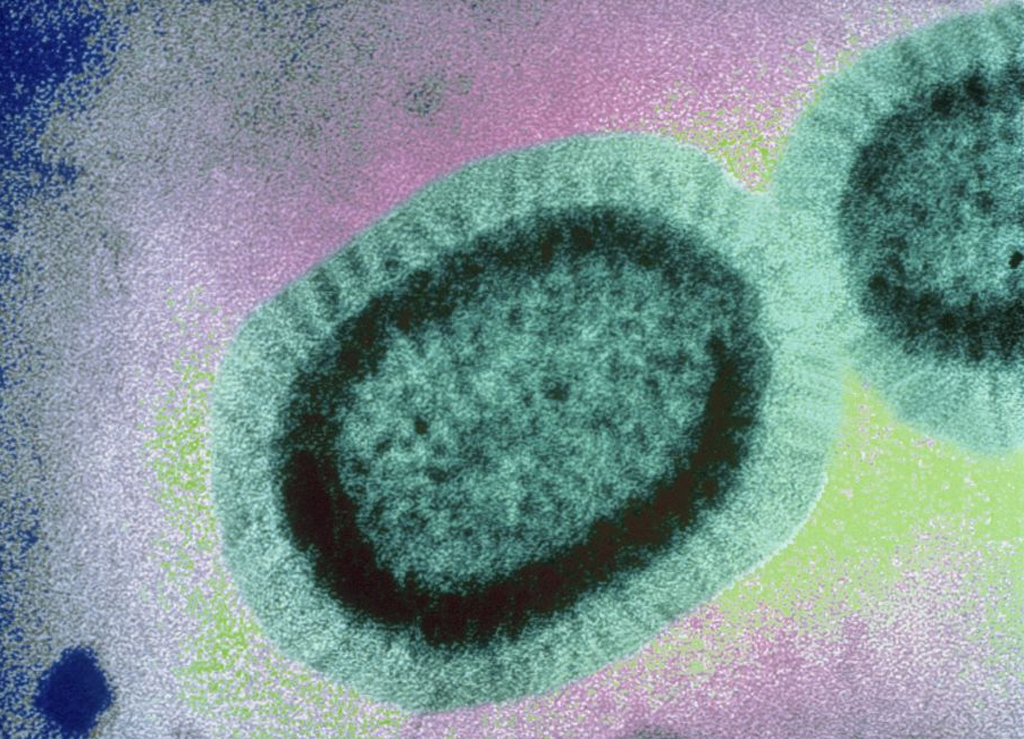
“We are no more in the aerosol camp than the contact camp” conclude the authors. And this seems to be how it is in terms of influenza transmission routes – you’re either in one camp or the other. This 2010 PLoS Computational Biology paper is hardly hot off the press, but it is important and it does, to an extent, put the question of which camp you are in for influenza transmission to bed: you need to pitch your tent in different camps depending on the circumstances.
The paper describes a model to compare the various transmission routes for influenza, principally airborne, droplet and contact. The study evaluates four transmission routes: ‘respirable particles’ (<10 µm), ‘inspirable particles’ (>10 µm, <100 µm), ‘direct droplet spray’ (>100 µm) and ‘contact’. The model tests 10,000 scenarios, considering possible variation in virus properties, host susceptibility and environmental factors (such as the number of influenza shedders).
The key finding is that contact transmission had the highest average basic reproduction number (R0) (1.7) followed by droplet (0.27), respirable (0.05) and inspirable (0.006) particles (Figure). However, that is only part of the story. Of the 10,000 scenarios evaluated, contact only was associated with high transmission in 3,069, all four routes in 342 and none in 4,765. In high host density settings, all routes were more frequently important. Conversely, when self-inoculation was more common (i.e. when simulated individuals touched their simulated nose, eyes and mouths more frequently), contact transmission was more important.

Figure: Basic reproduction number (R0) of four influenza transmission routes, ‘respirable particles’ (<10 µm), ‘inspirable particles’ (>10 µm, <100 µm), ‘direct droplet spray’ (>100 µm) and ‘contact’.
The findings are interesting and probably very important. It’s a shame they were not able to evaluate the relative importance of contact transmission involving contaminated surfaces compared with contact transmission that occurs independent of surface transmission (this has been evaluated elsewhere). Also, I remain suspicious of modeling in general. If simplifying assumptions are too simplistic (which is often the case), the model spits out garbage, which is worse than useless. Put another way, Bertha can produce anything if she’s given the right inputs! Plus, it’s difficult to know how applicable these findings are to other respiratory viruses.
Still, the paper does shed light on the relative importance of influenza transmission routes. Which is most important? Well, that depends on the context. If you’re in a small room, airborne and droplet transmission is key. If you’re admitted to a room following the discharge of a patient with influenza, then contact transmission is key. Hence, we need to be flexible when considering influenza transmission routes and ‘contextualize’ our interventions accordingly.
Image: Sanofi Pasteur.
How much Clostridium difficile infection is hospital-acquired? Part II
I wrote a blog last year on the excellent New England Journal of Medicine Oxford CDI study, which showed that a surprisingly high proportion (45%) of new CDI cases were genetically unrelated to recent CDI cases. This is not quite the same thing as evaluating how much CDI is hospital-acquired, mainly because the test used to detect CDI in the study has been phased out due to poor sensitivity, patients and staff were not screened for asymptomatic C. difficile carriage, and the environment was not sampled, so there was a large, unrecognized, hospital-based C. difficile reservoir from which horizontal transmission almost certainly occurred. A study published at the end of 2013 provides evidence that one of these potential reservoirs for transmission – asymptomatic carriage by other patients – is substantial.
The study was performed by a team from the University of Pittsburg Medical Centre. All patients screened for VRE during 5 months in 2009 were also screened for C. difficile carriage. Stool samples from symptomatic patients were also cultured. All toxigenic C. difficile were typed by multilocus variable number of tandem repeats analysis (MLVA). A total 56 C. difficile isolates from symptomatic CDI cases defined as healthcare-associated (HA-CDI) were available for typing. In addition, toxigenic C. difficile was identified in 226 (7.5%) of 3006 patients, and these isolates were also. Of the 56 HA-CDI isolates, 30% were genetically related to isolates from symptomatic cases, 29% to isolates from asymptomatic carriers, and 30% were unrelated to other isolates (Figure).

Figure. Proportion of HA-CDI cases genetically related to isolates from symptomatic cases, asymptomatic carriers and unrelated to other isolates.
The study provides a somewhat skewed view of asymptomatic C. difficile carriage since only patients considered at a high risk of carrying VRE were screened (admissions from other hospitals, ICU patients and long-stay inpatients). This meant that 75% of admissions were not screened for C. difficile carriage. Symptomatic cases are often described as the “tip of the ice berg”; in this study, three quarters of the ice berg remained submerged.
The authors performed an environment survey in the rooms of six asymptomatic C. difficile carriers and found that 5/6 rooms (48% of 25 sites) were contaminated with toxigenic C. difficile. And this is in a hospital that routinely uses bleach for disinfecting patient care areas! It’s interesting to note that transmission appeared to occur from the prior room occupant in 4/56 (8%) of HA-CDI cases, two of which were from asymptomatic carriers.
Another finding was that 158 patients had CDI diagnosed during the study period but 22% of these were counter-intuitively classified as carriers. This is perhaps because the lab performed a cytotoxin cell culture assay from both formed and unformed stools. We need to apply the “no diarrhea, no diagnosis” rule!
One other consideration is the molecular typing method used: MLVA. This is less discriminatory that the whole genome sequencing (WGS) used by the Oxford team. With WGS, strain relatedness is a question of how many single nucleotide variants (SNVs). With MLVA, it’s a question of distance of separation on a phylogenic tree. But you have the same fundamental problem: how do you define genetic relatedness? In reality, strain relatedness is an arbitrary line in the sand and our understanding of molecular clock speed is a work in progress.
So, is it time to screen and isolate asymptomatic carriers of toxigenic C. difficile? One of the arguments against this is that “asymptomatic carriers don’t have diarrhea, so therefore, don’t shed much C. difficile”. However, the environmental findings of this study, and others, suggest that asymptomatic carriers shed almost as much C. difficile as do symptomatic cases. I expect to see some controlled studies in the near future that should provide outcome data to help us to decide whether to pull the trigger on screening and isolation for asymptomatic carriers of toxigenic C. difficile.
Despite sampling only 25% of the asymptomatic carriage ice berg, apparent transmission from symptomatic CDI cases and asymptomatic C. difficile carriers was approximately equal. Plus, the study did not consider staff carriers or ancient environmental reservoirs. Thus, it seems that the large majority of C. difficile is acquired in hospital, but not necessarily from symptomatic CDI cases.
