A new JHI study highlights the dangers associated with reusable PPE, and related to PPE doffing in general. The study used a clinical simulation suite to monitor the spread of fluorescent material added to the outside of an N95 respirator during routine care for mannequin adult patients (with COVID-19!). Whilst some modes of PPE reuse were better than others, all of the clinicians involved in the study ended up contaminating the clinical environment with fluorescent material originating from the mask.
Continue readingPPE
COVID-19 and PPE: don’t forget your eyes!

One of the questions I get asked a lot is “where is the evidence that wearing eye protection reduces the risk of exposure to SARS-CoV-2, because it’s really annoying to wear and creates other risks related to reduced vision”. A new systematic review examines the effect of eye protection on reducing healthcare worker exposure to SARS-CoV-2. The short answer is that there is enough evidence to convince me that eye protection should be part of our SARS-CoV-2 PPE ensemble.
Continue readingTo FFP or not to FFP: variation in national guidelines on respiratory protection during the COVID-19 pandemic
Probably the most contentious aspect of the COVID-19 pandemic has been PPE for staff. And within that, the most contentious aspect of PPE has been respiratory protection when caring for patients with confirmed or suspected COVID-19: to FFP or not to FFP? I have been involved in a review of international guidelines to identify variation and track the changes in the guidelines over time. Things have changed as evidence has emerged, but international guidelines still disagree on where and when FFP respirators should be worn when caring for patients with suspected or confirmed COVID-19. The review also tracked variation and changes in recommendations about what should be considered an AGP.
Continue readingThe impact of a ward-based ‘PPE Helper’ programme on staff perceptions about COVID-19 PPE
During the first wave of COVID-19, we developed a ‘PPE Helper’ programme. This ward-based programme put PPE experts on the front line to spend time with staff to improve PPE knowledge, promote safe and effective use, and address staff anxiety. The programme was evaluated through a survey of staff views about PPE at the conclusion of the programme. This found that staff who had had contact with a PPE helper responded more positivity to questions about PPE and felt less PPE-related anxiety too.
Continue readingPlease, no gloves to prevent COVID-19

There are rumblings that glove wearing (aka “hand coverings“) are being considered as a widespread recommendation to prevent the spread of SARS-CoV-2 in public places (e.g. shops) in the UK. The message of this post is simple – please, no gloves. Convincing clinical staff of the unintended consequences of glove overuse is tricky enough. But widespread use of gloves in public places like shops may just bring me to tears. (Unless anybody can point me in the direction of solid evidence that this is likely to have a net benefit in reducing transmission…!).
COVID-19 & PPE / face coverings / masks / shields: personal safety depends on more than what you wear
There’s a huge amount of academic and pragmatic discussion and debate about the appropriate levels of PPE to wear in various healthcare settings to reduce the risk of spreading COVID-19 to yourself and others in healthcare settings. And more recently, when to wear face coverings / masks / shields in public areas of hospitals, on public transport, and in shops. However, there is much, much less discussion about the importance of careful doffing (removal) of PPE and face coverings etc in order to ensure the safe and effective use of PPE. This helpful Cochrane Review, updated for the COVID-19 era, covers a lot of ground and one key conclusion is that doffing is key: if it is done carefully, the risk of self-contamination is lower.
The case for face shields in preventing the spread of COVID-19

I’ve been meaning to write this post for a while. As UK government guidance has changed, face masks and face coverings will be very much the norm on public transport and in healthcare settings soon. So, now is a good time to consider whether face shields could play a role in preventing the spread of COVID-19.
COVID-19: Learning rapidly from an overwhelmed healthcare system in Bergamo, Italy
A very sobering piece published in NEJM Catalyst Innovations in Care Delivery (a new digital journal in the NEJM group) describes a catastrophic situation in a hospital in Bergamo, Italy, which has been overrun by COVID-19. We all have much to learn from this experience: about pandemic preparedness, response, and the key role of IPC at all stages of this pandemic.
PPE for preventing highly infectious diseases
The use of PPE and the protection of HCWs against highly infectious diseases was (and is) a topic of major importance, around the globe. The recent Cochrane review by Verbeek et al. was probably hoping to offer this “vital” information.
Unfortunately, they found no studies on the effects of goggles, face shields, long-sleeved gloves or taping on the risk of contamination. All they found was very low quality evidence, with high risk of bias and uncertain estimates of effect, that:
- More breathable types of PPE offer more comfort without increasing the risk of contamination
- Double gloving and CDC doffing guidance appear to decrease the risk of contamination, and
- Active more than passive training in PPE use may reduce PPE and doffing errors.
Their conclusions are obvious: we need high-quality studies of the materials, their use and protective effects, safe ways of doffing, and the most adequate training to achieve safe use of PPE for HCWs in the presence of highly infectious diseases or those (even less infectious) that may cause severe harm to HCWs.
But what to do until than? My personal opinion is that we should only use PPE, we are used to and know how to use. First-time users, even if supplied with the best available products, will inevitably fail to remove the PPE without error. Consequently, institutions should have a stable selection of PPE, and in the case of preventing highly infectious diseases, a selected group of HCWs with continuous active training, as it is too late to start when the next epidemic is hitting our healthcare centers.

Ebola: PPE and paranoia
The contrast in the stringency of the CDC and UK Department of Health / Health and Safety Executive guidelines for infection prevention and control when dealing Ebola virus disease (EVD) patients is striking. This is particularly acute with regard to recommendations for Personal Protective Equipment (PPE) and terminal disinfection. Having recently reviewed both documents for a webinar on Ebola infection prevention and control (you can download the slides here, by the way), I thought I’d share the contrast:
Table: PPE and disinfection recommendations for dealing with patients with Ebola virus disease. Source: US CDC patient and environmental guidelines, and UK Department of Health. (Please note – this summary chart is designed to be illustrative rather than definitive.)
So is there any reason why the level of PPE and type of terminal disinfection required should be any different depending on which side of the Atlantic you happen to be? None whatsoever. So why the discrepancy? It’s difficult to say. This difference in recommendations has prompted the question of “To CDC or not to CDC” in terms of PPE for Ebola, and an opinion piece in Annals of Internal Medicine justifying the CDC approach. It is probably true that the level of PPE recommended by CDC is enough to block transmission, and that the risk of environmental contamination is low enough such that fumigation is not necessary. Probably. But is that good enough when Ebola is on the line? It is certainly true that you can be wearing all the PPE in the world but if you put in on incorrectly, don’t take care of it during use or remove it carelessly you will put yourself at risk.
When I came to decontaminate a room using hydrogen peroxide vapour following a case of Lassa fever in London some years ago, I wore all the PPE that I could lay my hands on (see below)!
Me illustrating the “belt and braces” (aka paranoid) approach to PPE (a la UK, not CDC recommendations).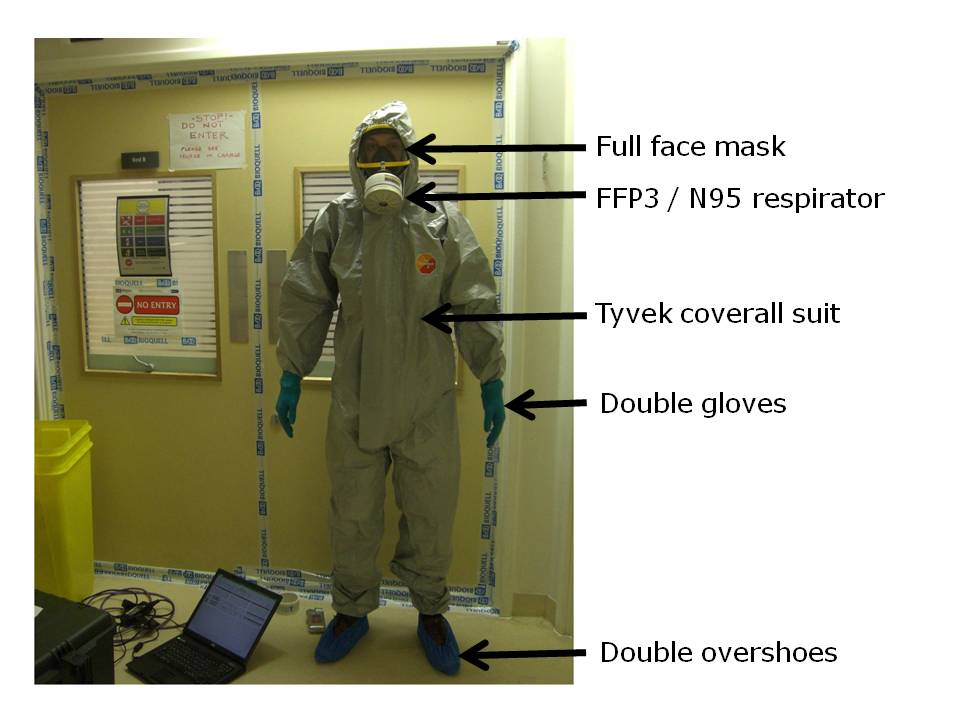
Did this level of PPE match the risk of exposure to viable Ebola? Perhaps not, but it certainly made me feel a whole lot more secure about entering the room to do the job!
