Just before Christmas a follow-up on that what bothers us most: patients dying because of antibiotic resistance. I previously tried, see here, to disentangle from the ECDC study (33.000 deaths per year in Europe) how they got to 206 AMR casualties in the Netherlands and ended with a recommendation to not “focus too much on the absolute numbers as they may not be very precise.” With Valentijn Schweitzer I spent some more time in the 200 pages supplement, only to find out – in the end – that the Americans do these kind of studies much better. Continue reading
VRE
Attacking the fecal veneer (part 2)
Last year (Jan 17, 2017) I blogged on an excellent pragmatic cluster-randomized crossover study in which 4 patient room cleaning strategies were tested for their effectiveness to reduce acquisition of bacterial carriage for the incoming patients. The authors’ conclusion was that “enhanced terminal room disinfection decreases the risk of pathogen acquisition”, which I interpreted as “Not for C. diff, may be for MRSA and yes for VRE.” Now the same group published the effects of these interventions on infection/colonization with these pathogens in ALL patients admitted to the hospital during the study period, see. Authors’ conclusion this time: “Enhanced terminal room disinfection with UV in a targeted subset of high-risk rooms led to a decrease in hospital-wide incidence of C difficile and VRE.” Really? Continue reading
No more antibiotics for animals
That’s what the WHO stated this week, and it was based on a study, in Lancet Planetary Health. In most news items that I saw animal antibiotic use was directly linked to human infections caused by antibiotic resistant bacteria. A journalist even asked if eating meat was safe. Although most of us (including me) support reduction of unnecessary antibiotic use, it’s worth reading this excellent meta-analysis, initiated by WHO. Did this study answer the burning research question “to what extent does animal antibiotic use influence infections in humans?“ Continue reading
VRE: MRSA or MRSE?
To me, VRE is an old love that never let me down. In 1995 (!) I studied its epidemiology in Chicago (using PFGE), and we described it as the “triple-threat bug”: a gut colonizer like Gram-negatives, a skin colonizer like MRSA and an environmental contaminator like C. diff. A new study in CID, using WGS, illustrates its complex epidemiology. After 20 years, that complexity seems explained, and now we can no longer avoid the question what to do with VRE. Keep on cherishing its “feared pathogen status” like MRSA, or accept that it is just something like MRSE, and stop bothering. Continue reading
Attacking the fecal veneer*
What an excellent start of 2017. A great study from the USA today in Lancet: In a pragmatic cluster-randomized crossover study they tested 4 patient room cleaning strategies on the effectiveness to reduce acquisition with relevant bacteria for the incoming patients. The conclusion states that “enhanced terminal room disinfection decreases the risk of pathogen acquisition.” Yet, this paper is so “data-dense” that you must read the methods (and supplements) to get the picture. In one shot: Not for C. diff, may be for MRSA and yes for VRE. Continue reading
What do you do to prevent VRE transmission?
What do you do to prevent VRE transmission?
…you are not alone, if the answer to this question is ‘nothing special’, based on survey published in ARIC! Dale Fisher’s team in Singapore put together a simple survey, asking the global IPC community what measures they have in place to prevent the transmission of VRE. There was a huge degree of variability, ranging from ‘nothing special’ to ‘the kitchen sink’!
Survey: infection prevention practices for VRE

Guest post from Prof Dale Fisher (bio below). Please help Dale out by completing this survey. I found it interesting (and more importantly, quick)…
This study has been BUGGing me for a while

A fabulous study recently published in JAMA evaluates the ‘Benefits of Universal Glove and Gown’ (BUGG) in US ICUs. This is a model study design: one of the first cluster randomized controlled trials of a non-therapeutic infection control intervention. Twenty ICUs were paired and randomized to either universal glove and gowning, or to continue the current practice of placing patients known to be infected or colonized with MRSA and VRE on contact precautions. The hypothesis is that undetected colonization with MRSA and VRE is common, and the only real way to address this is to assume everybody is colonized!
Summary of findings:
- Universal glove and gowning was not associated with a reduction in a composite measure of MRSA / VRE acquisition (the primary outcome).
- VRE acquisition was not reduced by universal glove and gown use, whereas MRSA was.
- CLABSI, CAUTI and VAP; ICU mortality; and adverse events did differ significantly between the two groups.
- Hand hygiene compliance on room entry was not significantly different between the two arms, whereas hand hygiene compliance on room exit was significantly higher in the intervention arm.
- Healthcare workers visited patients 20% less frequently in the intervention arm (4.2 vs. 5.2 visits per hour).
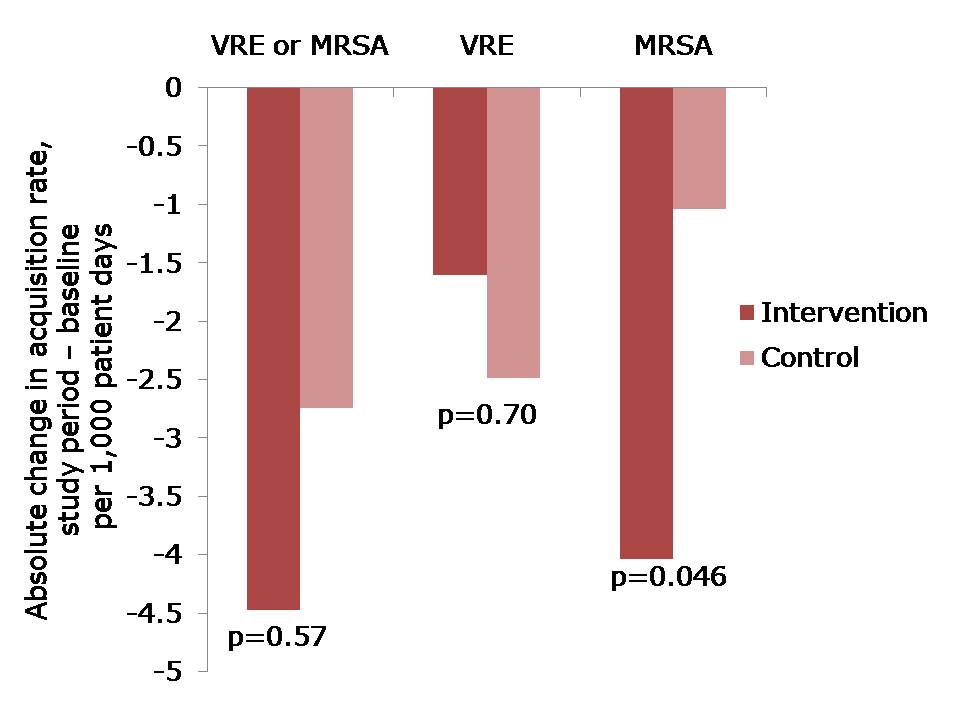 Figure: The change in acquisition rate, comparing the baseline period with the study period for the intervention and control units.
Figure: The change in acquisition rate, comparing the baseline period with the study period for the intervention and control units.
Here’s what’s BUGGing me about this study:
- The acquisition rate in both intervention and control study arms reduced (Figure). The acquisition rate reduction in the control arms may be due to improved compliance with admission screening, resulting in more accurate ascertainment of who required contact precautions.
- The significant reduction was achieved for MRSA but not for VRE. The authors suggest that VRE colonization may have been suppressed on admission and not detected, and flourished during antimicrobial therapy giving the impressive of acquisition. I wonder whether differences in the routes of transmission may also have contributed; for example, VRE seems to be substantially “more environmental” than MRSA. Another potential confounder is that, by chance, the prevalence of MRSA or VRE on admission to the intervention ICUs was more than double that in the control ICUs (22% vs. 9%). In actual fact, the raw rate of MRSA acquisition in the intervention ICUs was marginally higher than in the control ICUs during the intervention period (6.00 vs. 5.94 per 1000 patient days), even though the change in rate was significantly greater on the intervention ICU. Although adjustment was made for this difference in the analysis, it may have skewed the findings somewhat.
- The authors achieved remarkably high compliance with admission screening (around 95%), discharge screening (around 85%) and glove and gowning (around 85%). Each site had the luxury of a study coordinator and a physician champion to lead implementation, plus weekly feedback on screening compliance and visits from study investigators. Most ICUs would not be afforded these luxuries so I suspect that real-world compliance outside of the somewhat artificial study environment would be considerably lower. Indeed, an ID Week poster suggests that compliance with gowning in one US ICU was a ‘dismal’ 20%!
- Adverse events were not significantly higher in the universal glove and gowning arm, which may seem surprising prima facie. However, the reason why adverse events are more common for patients on contact precautions is that they are marginalized by being on contact precautions. If all patients are effectively on contact precautions, the time of healthcare workers would be spread evenly.
- Universal gloving is likely to result in universally bad hand hygiene compliance within the room during patient care; when healthcare workers feel protected, they are less likely to comply with hand hygiene and gloves are a good way to make healthcare workers feel protected. The increase in hand hygiene compliance on room exit is probably also a symptom of inherent human factors, since healthcare workers feel more ‘dirty’ when exiting the room of a patient with a higher perceived risk of MDRO ‘contamination’ (the so-called “urgh” factor).
- Healthcare workers had less time for patient care in the intervention arm because they were busy donning and doffing gloves and gowns. Interestingly, the authors suggest that fewer visits may be a good thing for patients, and may have contributed to their reduced chances of acquiring MRSA. This seems unlikely though, given the fact that VRE acquisition was not reduced. On balance, less contact with healthcare workers is likely to be bad for patients.
- The increased cost of universal glove and gowning was not evaluated and, whilst incrementally small, would be a substantial sum.
In summary, this study sets the standard in terms of rigorous assessment of an infection prevention and control intervention. Universal application of gloves and gowns is unlikely to do as much harm as universal administration of mupirocin, but it will not make a profound reduction in the transmission of MDROs. Therefore, I shouldn’t think many ICUs will be rushing to implement universal gloves and gowns on the strength of these findings.
