Just before Christmas a follow-up on that what bothers us most: patients dying because of antibiotic resistance. I previously tried, see here, to disentangle from the ECDC study (33.000 deaths per year in Europe) how they got to 206 AMR casualties in the Netherlands and ended with a recommendation to not “focus too much on the absolute numbers as they may not be very precise.” With Valentijn Schweitzer I spent some more time in the 200 pages supplement, only to find out – in the end – that the Americans do these kind of studies much better.
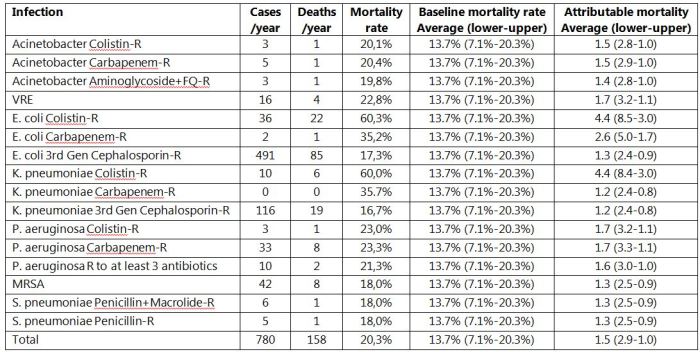
First, the ECDC study. All the work boils down to a product of 2 estimates: the number of infections caused by a resistant bug and the extra risk of dying from that infection because of the resistance. For simplicity we have focused on bloodstream infections (BSI). The first surprising thing is that they used the same baseline mortality rates for BSI caused by any “susceptible” pathogen, whether it is E. coli, S. pneumoniae or an enterococcus, which ranged from 7.1% to 20.3% with an average of 13.7%. Then there are 16 bug-drug combinations for resistance. For E. coli there are 3: colistin-resistant, carbapenem-resistant and 3rd generation cephalosporin resistant. BSI caused by these resistant pathogens have a higher mortality (for these 3 being 60%, 35% and 17%, respectively). The ratio can be seen as the attributive mortality; being 4.4, 2.6 and 1.3 for these 3 respectively.
Valentijn calculated figures for the Netherlands and these are in the Table. With that information we have recalculated how the investigators came to the 206 deaths in the Netherlands, of which 158 would die after AMR-BSI. To read the Table: For VRE the average risk to die from a Vancomycin-susceptible enterococcus BSI is 13.7% (ranging from 7.1% to 20.3%) and this risk is 22.8% in case of VRE, which corresponds to an average attributive mortality of 1.7 (ranging from 1.1 to 3.2) yielding 4 deaths per year as we have 16 of such episodes.
As mentioned in the previous blog we were surprised to see deaths occurring from colistin-resistant E. coli, as I never encountered such infections yet. Well, we do, and the investigators have explained that these colistin-resistant E. coli were susceptible – at least – to carbapenems. Yet, patients with infections caused by such bacteria would never be treated with colistin (unless allergic to all other classes of antibiotics). The 60% mortality (attributive mortality being factor 4.4) for such infections simply cannot be realistic and the true mortality due to colistin resistance in E. coli is likely zero. So, we should subtract 22 BSI deaths from 158.
For 3rd generation cephalosporin resistant E. coli and K. pneumoniae BSI attributive mortality rates were 1.3, where our own data come to an estimate close to 1. If the latter were true, we should subtract another 104. And with same reasoning another 12 for VRE and MRSA. Then we are at 20, that’s a relative difference of 87%.
Now, why are we making this so complicated? Wouldn’t it be nice if instead of a 12-page manuscript and more than 200 pages supplement we could have a results section of just a few lines? Yes, it would and it is possible and published:
Take the number of deaths in the country (USA) being 2,468,435 of which 715,000 die in hospital. With 34.4% of inpatients dying from sepsis (conservative estimate) and a reported rate of MDR pathogens in sepsis of 28.8%, MDRO sepsis caused 70,837 inpatient deaths each year. The other 1,753,435 are outpatient deaths. If you subtract deaths that are unlikely to be due to infection (e.g., suicides, accidents, and homicides) (N=180.811) and deaths due to infections (N=22.088), 1,550,536 deaths remain. If 17%–19% of these are due to infections (despite not being indexed as such) and – again – 28.8% are due to MDROs, there would be 285,680–316,690 deaths in which infection contributed to death, of which 82,276–91,207 deaths were due to MDROs. So, that makes 153,113–162,044 deaths because of AMR in the USA. All info is based on ICD-10 codes. The obvious fatal flaw in this calculation is that every patient dying with AMR is considered to be dying due to AMR, as if they all would have survived sepsis due to non-MDR pathogens. Concepts as attributive mortality make things unnecessary complex, leading to fake science, they must have thought.
With such figures and knowing that resistant bacteria (and genes) don’t respect borders they will need a much bigger wall for protection. If you think this was published in the BMJ Christmas edition, you’re wrong. It is in Infection Control and Hospital Epidemiology (online since Nov 22).
To end the year 2018! We still have to learn a lot about the true burden of AMR. So enjoy the holidays, we will be back with more on this topic in 2019!
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
