I heard an eye-opening talk at IPS about the cost of HCAI-related litigation to the NHS. This is something that gets talked about a lot in economic analyses (“these figures do not include the cost of litigation”), but it is difficult to find accurate figures on the scale of the expense. Data from NHS Resolution* suggests that HCAI-related litigation costs the NHS in the region of £60m per annum, which accounts for around 4% of all harm settlements from NHS Resolution each year.
NHS Resolution (previously the NHS Litigation Authority) is in charge of managing litigation related to clinical negligence / harm. In the last financial year (2016/17), there were 10,686 claims totalling £4.4bn, of which in excess of £1.6bn was paid out. Whilst the presentation did not include HCAI-related payments for 2016/17, the average HCAI-related annual payment between 2011/12 and 2015/16 was £57m, which equates to 3.6% of the 2016/17 total. The total annual payments for HCAI-related litigation have fluctuated a little but not risen dramatically (see Figure 1).
Figure 1: Trends in total HCAI-related litigation costs. These are total payments made in each financial year, which may not necessarily be linked to cases reported in the same year, and which may be include regular payments for long terms conditions related to harm.
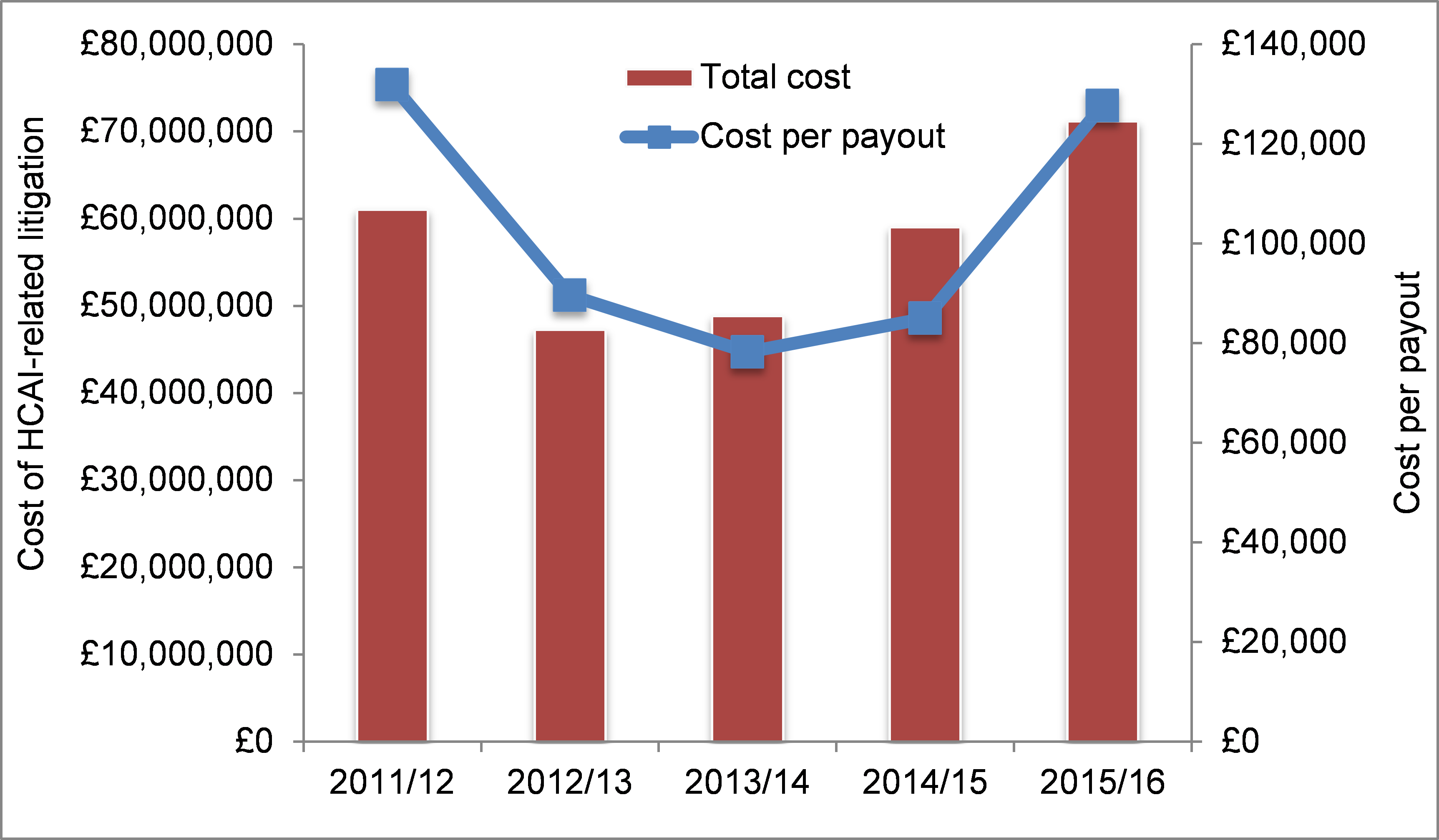
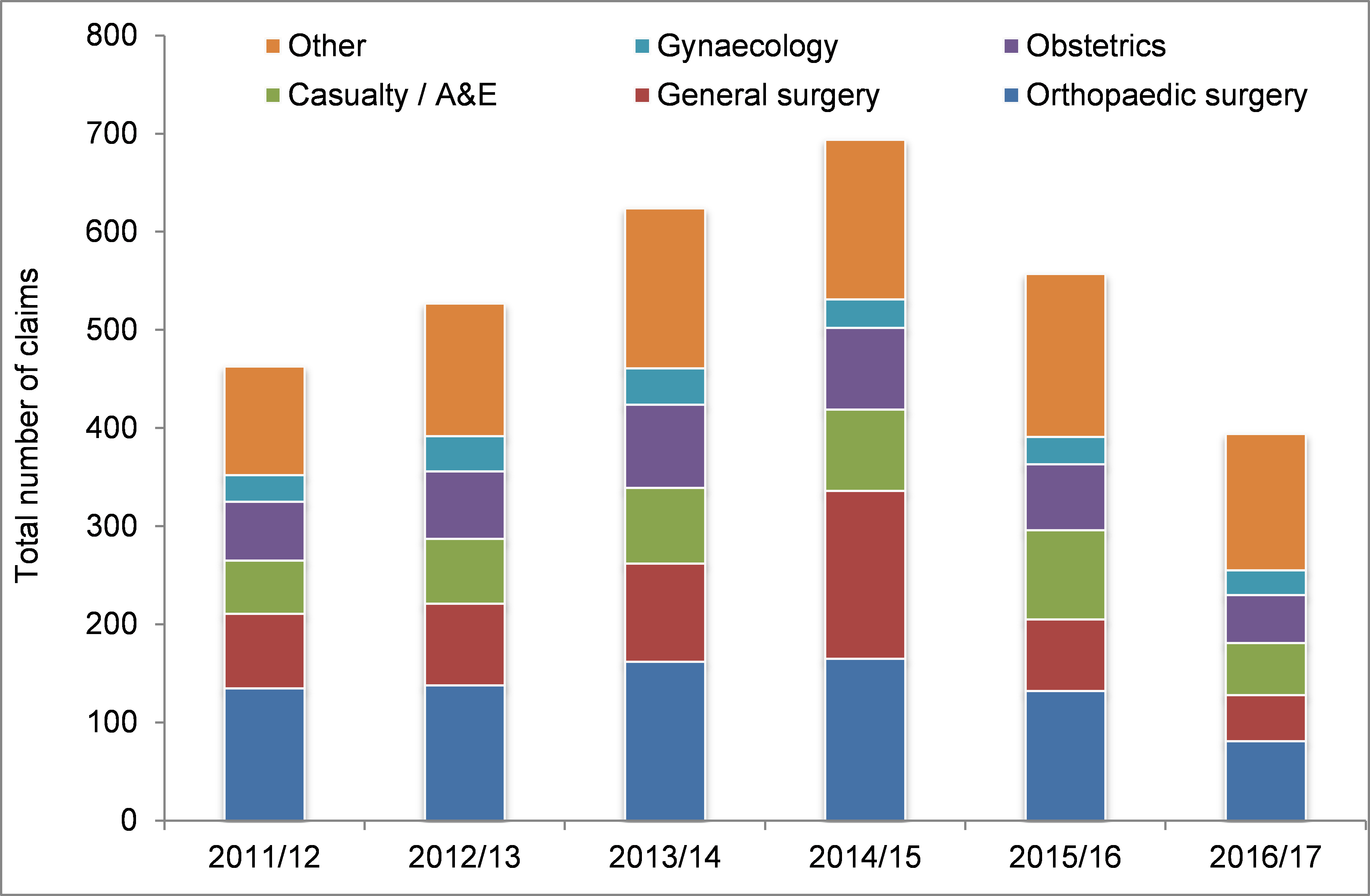
There’s an interesting trend in the total number of HCAI-related claims, which rises to peak in 2014/15, then declines to almost half the 2014/15 total in 2016/17 (Figure 2). This may be because there is a delay in the incident occurring and a claim being registered. This means that the average cost per payout is looking higher in recent years, but would reduce if the number of claims does rise (see Figure 1). Overall, the most common source of HCAI-related litigation is orthopaedics (around 30%) followed by general surgery (around 20%), then A&E (around 15%) (Figure 2). These proportions have not changed much over the past five or so years.
Figure 2: Number of claims per annum, including breakdown by speciality.
As ever, these are some limitations / caveats to the dataset. Claims are not generally labelled “HCAI”: Tracy ran a sensible series of search terms to pull out HCAI-related claims, but some HCAI-related claims may have been missed. Also, there will be cases where HCAI was a contributing factor, but not the final reason for the claim. Taken together, this probably means that the total cost of HCAI-related litigation is under-estimated.
NHS Resolution have recently released a five year strategy: ‘Delivering fair resolution and learning from harm’, which looks to be a very positive direction. The centre piece of the strategy is to handle harm better when incidents occur to reduce the chances of a situation becoming litigious later on. Human patients are willing to accept that human care givers will make mistakes – how these mistakes are handled and communicated is crucial. I was once on the receiving end of a pretty serious medication error in a different country (I’ll tell you over a beer sometime), which was handled pretty well. NHS Resolution are also doing some good work to prevent and improve the management of sharps injuries, which is worth a look.
I hope that this post will be helpful in arming us with the data that we need to highlight the true cost of HCAI to our organisations. Indeed, a previous attempt published some years ago by colleagues at Guy’s and St. Thomas’ reported a scale of HCAI-related litigation (£25k over three years) that was a couple or orders of magnitude lower than the figures reported here. Counting the cost of CPE outbreaks is all well and good, but it seems that the cost of HCAI-related litigation makes a significant contribution to the total financial burden of HCAI. Finally, I would like to say thank-you to NHS Resolution for giving me permission to share these numbers, and helping me to understand them.
* Thanks to Tracy Coates from NHS Resolution for sharing her slides and giving me permission to include figures on this blog.
Image: Flickr.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

One further uncounted and perhaps uncountable cost is that of the internal investigation. This is certainly onerous in terms of responding to legal questions and finding x, y and z pieces of information. Also in meetings to pass on information and findings of the investigations. One litigation which took several years to come to a conclusion (which the claimant lost) impacted significantly in time away from infection prevention.
Question: In an era of decreasing HAI (according to PPS) why is the amount awarded increasing?
Question2: Is the cost per pay out increasing > the rate of inflation, if so are the infections more serious or the payouts more generous/realistic.
As always with data…. you need more data…
LikeLike