Overall 61 colleagues from 17 countries answered the questionnaire. A large proportion (26 of 61) of the answers came from the UK, which might have to do with the fact that the first European outbreak was described in England.
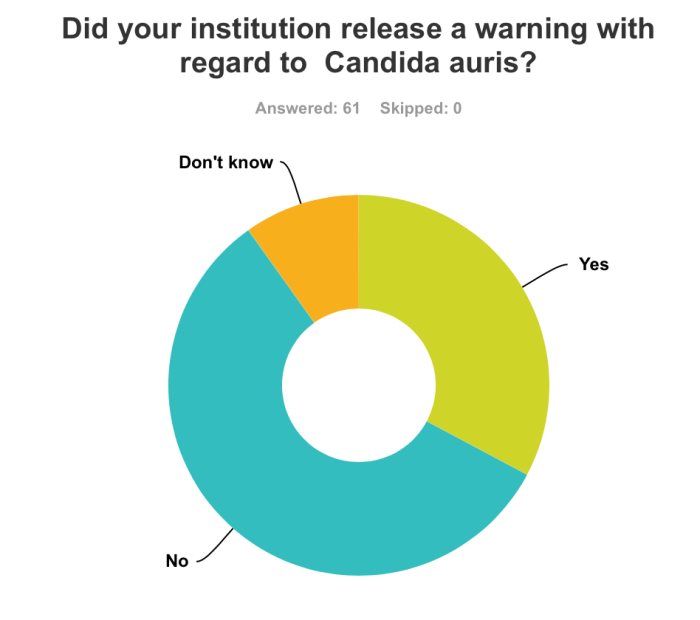
Of the respondents 32.8% said that their institution released a warning about C. auris. Analyzing the data separately for the UK and the other participating countries, it became clear that the first European outbreak had impact on the preparedness. In the UK 42.3% of the institutions were warned about the unique capacities of C. auris, versus 25.7 in all other countries. Regarding the existence of a written guideline dealing with C. auris, the differences were far less pronounced, namely 26.9% versus 20.0%, respectively.
53.9% of the UK responders believe that their lab can correctly diagnose C. auris, versus 31.4% in the other countries. In addition, the proportion of responders, who didn’t know if their lab was prepared, was higher outside the UK (45.7% versus 26.9%, respectively).
Despite the emerging spread of C. auris clusters this questionnaire is an indication that most institutions are not adequately prepared. Obviously the sample is really small, but the outcome was predictable. With an increasing body of literature, including papers on diagnostic methods and infection control measures, we should hope that the situation should change very soon. Thus, don’t lean back, start writing.