As the outbreak of Ebola continues unabated in Sierra Leone and Liberia (1323 cases and 729 deaths as of July 27), I thought it would be an opportune moment to share a close shave that I had with the closely related Lassa viral haemorrhagic fever (VHF) virus in 2009.
As the outbreak of Ebola continues unabated in Sierra Leone and Liberia (1323 cases and 729 deaths as of July 27), I thought it would be an opportune moment to share a close shave that I had with the closely related Lassa viral haemorrhagic fever (VHF) virus in 2009.
A patient was transferred from Mali to a London hospital with a diagnosis of malaria. The case was initially thought to represent a low risk of VHF (to be fair, Lassa had never been reported in Mali, and the patient came with a diagnosis of malaria). This led to the potential exposure of 123 healthcare workers and visitors, and a busy week for the infection prevention and control team to follow each of these individuals. The useful risk assessment now available from Public Health England may have helped to reduce the number of people exposed.
The patient died in a negative pressure ICU room on the day of admission. At that time, there were no clear recommendations about how to decontaminate the room, so I was involved in developing a decontamination plan with the hospital. Due to the rarity of VHF in the UK, the plan took a week to be authorized by the Health and Safety Executive. This meant that by the time it came to decontaminating the room, the bags of blood-soaked clinical waste, spots of blood on the bed, and used consumables on the floor had been festering for a week. Not ideal.
Our decontamination plan included the use of hydrogen peroxide vapour (HPV) for terminal room disinfection due to the risk that VHF viruses can survive when protected by blood for several weeks on surfaces. This is borne out by some sampling during an outbreak that found intact RNA from the Ebola virus on blood contaminated fomites (although not on fomites that were not contaminated with blood). It’s reassuring that the Department of Health / Health and Safety Executive guidelines published a few years after this case also recommend the use of fumigation for terminal decontamination of hospital rooms.
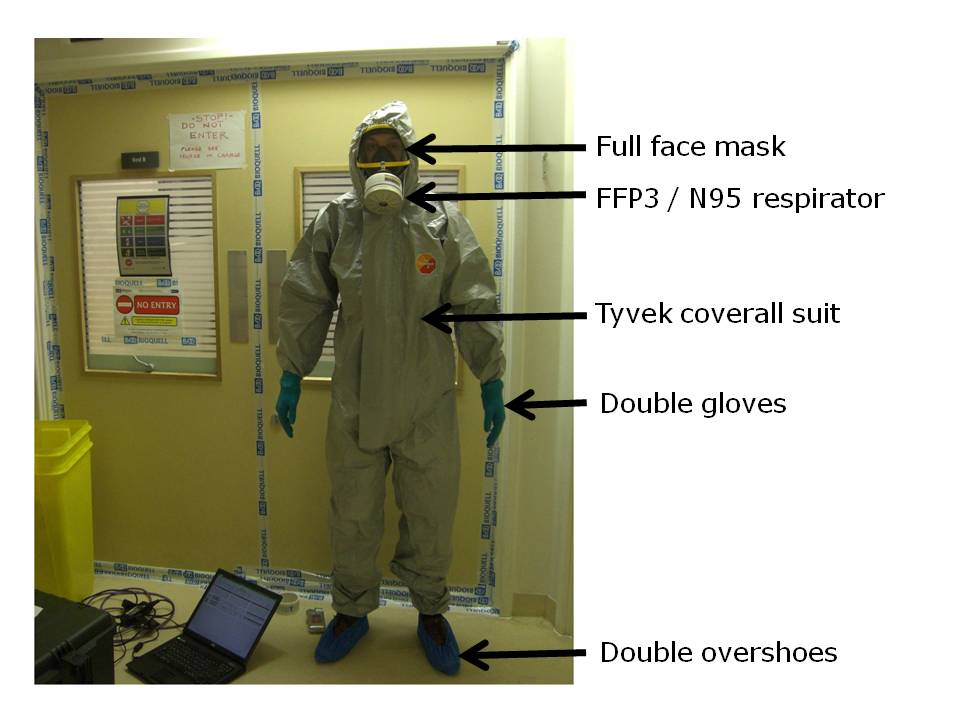
I ended up being tasked with setting up the HPV equipment that was used to decontaminate the room. We decided it would be better to clean the room after the decontamination to provide some protection to the cleaners. This meant that I was the first person to enter the room after the body of the patient had been removed. I will never forget donning my Tyvek suit, gloves and face-fitted FFP3 mask (see below!). It was exciting: I felt a lot like Dustin Hoffman in Outbreak (the movie that got me interested in medical microbiology in the first place). But it was also frightening. The most frightening part was collecting the bags of clinical waste and consumables from the floor, knowing that they were still likely harbouring live Lassa fever virus. To think that one slip could have infected me with a deadly virus for which there is no treatment…

Figure: Me kitted out in PPE (and looking somewhat apprehensive)
There is legitimate concern that we may see cases of Ebola in the UK and USA in this globalized, interconnected world. If so, then we need to be prepared, and some have questioned our state of readiness. We are fortunate to have comprehensive guidelines from the Department of Health / Health and Safety Executive, including clear guidance on how to decontaminate a room following a case of VHF.
My close shave with VHF has given me a great deal of respect and, frankly, veneration for the brave healthcare workers who are risking their lives on the front line in bringing the current outbreak of Ebola under control.
Photo: Ebola courtesy of Phil Moyer and CDC/Cynthia Goldsmith.
 It’s been another busy quarter on the Micro Blog, with posts on Ebola, coverage of Infection Prevention 2014, and updates on multidrug-resistant Gram-negative rods (especially CRE):
It’s been another busy quarter on the Micro Blog, with posts on Ebola, coverage of Infection Prevention 2014, and updates on multidrug-resistant Gram-negative rods (especially CRE):