As England moves away from confirmatory PCR testing following a positive lateral flow test in the absence of COVID-19 symptoms, it’s a good time to look at what these two different testing strategies can offer us. There’s an excellent short review in NEJM combined with a case study to help illustrate the impact of pre-test probability plays out. Both lateral flow testing and PCR testing have their place, and in some ways lateral flow testing is a better correlate for infectivity (as well as being cheaper and easier!).
The image below from the article provides a superb overview of how levels of virus, antigen, and antibodies change over time. (PCR detects viral RNA, lateral flow tests detect viral antigen, and blood tests detect antibodies.)
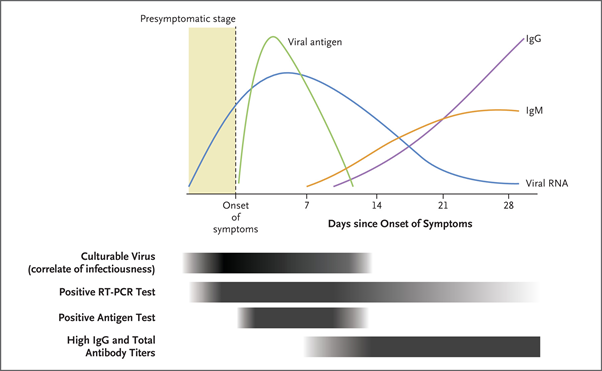
The period during which culturable virus can be detected seems to be a pretty good correlate with the period during which a patient is infectious. This is typically for a couple of days before the onset of symptoms (if there are any) until about 10 days after symptoms. As you can see from the chart, lateral flow testing is a better fit for this period than PCR testing, although won’t detect early infectivity. For me, this means that if a lateral flow test is positive, then the person is likely to be shedding culturable virus and to be infectious (to some degree). If a lateral flow is negative but a PCR is positive, you need to know when you are at the start of the end of the disease to inform decision making about infectivity (repeated PCR tests, an evaluation of CT values, and antibody testing can help here). An assessment of ‘infectiousness’ is more than what our diagnostic tests are telling us – we need to consider patient and environmental factors too. But both PCR and lateral flow testing are useful tools.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

Do you have evidence for this statement: “The period during which culturable virus can be detected seems to be a pretty good correlate with the period during which a patient is infectious.”? I do not mean this sarcastically, I would truly love to see empirical evidence. We have seen good correlations between nasopharyngeal viral load and both virus culturability and antigen test positivity, but I have no idea below which viral load we can assume viral transmission to be negligible, even in situations in which people are packed close together in a poorly ventilated room.
LikeLiked by 1 person
Great comment, thanks. Useful summary of the evidence from CDC here: https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html
LikeLiked by 1 person
Thanks, but this CDC guidance does not include the presymptomatic phase of infection. I am mostly interested in that phase because we know that transmissions by presymptomatic individuals do occur and these individuals have no idea that they are infected because they have not (yet) been ill (as opposed to individuals who are in the tail-end of their illness). In any case, will keep looking for empirical evidence!
LikeLiked by 1 person
Can we truly believe that negative lateral flow means not infectious? Does the whole idea of people being infectious 48 hours prior to the onset of symptoms also go away if we get a negative LFT? Negative LFT but positive PCR still signifies not infectious? Trying to understand how to do contact tracing for positive employees since we are now doing LFT for symptomatic employees but allowing them to work pending PCR results.
LikeLiked by 1 person
Useful comment thanks. I certainly don’t think that negative lateral flow means non-infectious or that positive lateral flow means infectious. My point is only that lateral flow testing is probably a better correlate of infectiousness than PCR
LikeLiked by 1 person