As we begin to look to the other side of the peak of COVID-19, this issue of more widespread testing of patients, staff (and indeed the general population) for infection with the SARS-CoV-2 virus whether or not they have symptoms is looming large. We need to think carefully about the risk of false positives when interpreting the meaning of a positive PCR test in a group of people with a low prevalence of SARS-CoV-2.
To this point in the UK, most testing has been focused on those with symptoms (patients admitted to hospitals, community cluster investigation, staff off work with symptoms). However, these a lot of discussion currently about how far to extend testing to include patients, staff, and members of the general public who have no COVID-19 symptoms. There’s a lot of logic to doing this – there’s undoubtedly a pool of asymptomatic and pre-symptomatic SARS-CoV-2 infected individuals who are contributing to transmission.
There’s an excellent BMJ article on how to interpret a positive test result here. In this article, the focus is on testing patients with symptoms for COVID-19 and therefore a higher pre-test probability of having the disease. In this case, false negatives (where the test is negative but the patient has the disease) are the concern. However, when using the same test for a patient who does not have symptoms and therefore the pre-test probability is lower, the scenario switches and a false positive comes into play – possibly in a big way.
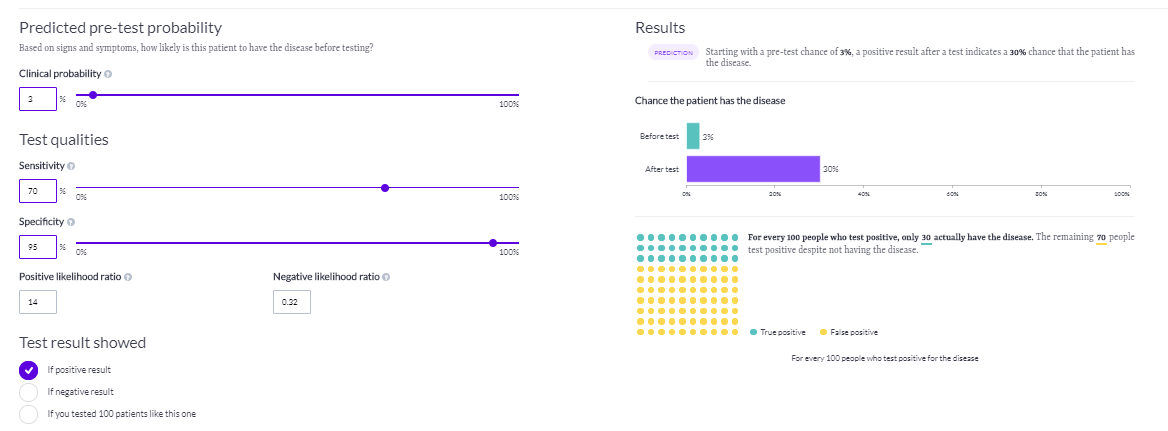
So, how would the commonly used RT-PCR tests fare for this? Let’s run through a scenario of testing asymptomatic staff, and assume the rate of positivity is 3% (based on this study). If we assume the sensitivity of your PCR is 70% and the specificity is 95% for illustrative purposes (these were used in the BMJ article), and a prevalence (aka pre-test probability) of 3%, then false positives are a major concern (see Figure 1, from here). Only 30 in 100 positive results will be true positives!
Figure 1: The probability of a PCR test returning an accurate positive result if the pre-test probability is 3%, and the assay sensitivity is 70% and specificity is 95%.
I think that in reality the specificity of the PCR assay is much better than 95%. So, let’s re-run this with a specificity of 99.5% (see Figure 2). In this scenario, it’s better but far from perfect: 81 in 100 positive results will be true positives, but you will still have 19 in 100 false positives.
Figure 2: The probability of a PCR test returning an accurate positive result if the pre-test probability is 3%, and the assay sensitivity is 70% and specificity is 99.5%.

There are some important implications here. If we are screening a large number of patients and staff without symptoms, a fair chunk of positives will be false positives. Therefore, it would not be wise to pluck an asymptomatic patient with a single positive PCR test and place them into the middle of a clinical area being used to care for patients with confirmed COVID-19. Equally, it would not be wise to leave them in the middle of a clinical area being used to care for patients without COVID-19 symptoms. Therefore, a move to a single room and a repeat test may be the way to go. You can decide for yourself how to manage a member of staff without symptoms but with a positive test result!
And let’s not forget the possibility of false negatives. In both of the scenarios above, the possibility of a false negative result is <1%. But even <1% can become a sizable number in a large screening programme.
There’s a lot of uncertainty here. How do we define a “gold standard” test for COVID-19 (you can’t grow it on an agar plate in the same way you would a bacterium)? How does the assay specificity and sensitivity vary across different PCR tests? What is the prevalence of asymptomatic infection in patients and staff, and how does this vary across different patient and staff groups? All of these factors will influence – and could even transform – how the scenarios above work out.
There is much current discussion and debate about whether to test patients and staff without symptoms for COVID-19 infection. I don’t think a high false positive necessarily argues against testing patients and staff without symptoms for COVID-19 infection, but it does argue for caution in interpreting the meaning of a positive PCR test result in a patient or member of staff without symptoms of COVID-19.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

In particular rather than “you decide” a false positive should be treated as a positive with several re-tests while isolated or with quarantine until a reliable test, or time, indicates differently.
As to false negatives some labs believe tests are not effective until at least the 4th day after exposure and contracting the virus while still asymptomatic. This means that a negative test result during that period is no longer subject to a 99.5% or other specificity but instead throws the results out the window.
With that timing scenario mitigation may mean interview to see if lifestyle, contacts, etc., are high or low risk and that’s a time to “you decide”. If one is protecting an elder or high medical risk person from transmission then the interview may make all the difference.
Is the person to be tested basically or completely isolated as modus apparandus during these times or is it an ICU nurse or otherwise at-risk activities, high number of contacts with people of varying interactions?
With 99.5% specificity excepting the initial 3 days of exposure model a person who is at low-risk is likely to have a true negative. By the 4th day (per what some labs are saying) the negatives can give reassurance.
Best wishes!
LikeLike