An unusual and interesting outbreak of CPE was published recently in Clinical Infectious Diseases. Several key points: don’t rely solely on a PCR detecting the “Big 5” carbapenemases (NDM, KPC, OXA-48, IMP, VIM) – at some point you need to test for phenotypic carbapenemase activity; WGS can really help us in unravelling complex transmission routes; and covert plasmid propagation within and between species is a reality.
The story begins with a resistant Klebsiella oxytoca urine isolate from which WGS unexpectedly detected an unusual carbapenemase, GES-5, months after the urine specimen was collected. This prompted the development of a GES-5 PCR, which was used in the detection of second cluster of 11 GES-5 producing K. oxytoca carriers. This discovery prompted a laboratory lookback, which identified a cluster of three GES-5 producing K. oxytoca (including the original urine isolate) about a year previously in different parts of the hospital. The isolates from the three patients in the first cluster were more diverse in terms of SNPs than isolates from the 11 patients in the second cluster; this suggests that undetected GES-5 producers were around at the time of the three clinical isolates in the first cluster.
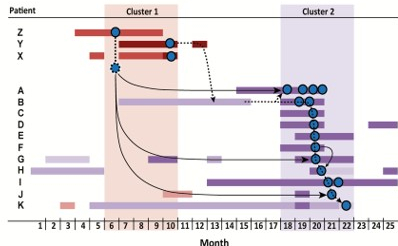
One of the patients in the second cluster had a very long hospital stay, and was an inpatient during the time of the first cluster – so, it was assumed that this patient linked the two clusters together (see the Figure). However, WGS told a different story – that an ‘unidentified genome’ (or series of genomes) were the link between the two clusters. This ‘unidentified genome’ could have been a patient, environmental reservoir, or possibly even a staff reservoir (although let’s not go there…!).
Figure: The two clusters of GES-5–producing Klebsiella oxytoca ST 138. The dotted lines show assumed transmission routes, but the black arrows show the transmission route supported by WGS which are different to those assumed epidemiologically and involve an ‘unidentified genome’ (the fuzzy-edged circle).
GES-5 was also detected in a handful of other bacteria elsewhere in the hospital through a prospective screening programme (2 x E. coli and 1x E. cloacae). Whilst the sequence of the GES-5 plasmid reported elsewhere are highly variable, all of the GES-5 producers had identical plasmids, suggestive of horizontal gene transfer. Furthermore, some other GES-5 isolates identified from diverse parts of the UK also carried the same plasmid, suggesting that this is part of a much wider picture of covert plasmid propagation!
Some reflections:
- Don’t rely solely on PCR to detect CPE; you need to have a phenotypic approach at some point along the diagnostic pathway, otherwise you risk missing unusual and non-standard carbapenemases.
- Don’t rely solely on clinical cultures to detect CPE – you need some sort of screening programme to keep on top of CPE. The first cluster had 3 clinical cultures positive for CPE, whereas the second cluster looked worse because it had 11 patients involved – but all bar one were CPE carriers only without positive clinical cultures.
- Apparent epidemiological links are easy to spot, but may not always tell the whole story. The unravelling of a simple picture of transmission to be replaced by a more complicated one, as was the case in this outbreak, is reminiscent of the CPE outbreak reported famously from the NIH Clinical Center – one of the first and best illustrations of how WGS can support and enhance outbreak investigations.
- It seems very likely that horizontal transfer of this GES-5 carrying plasmid occurred between species during the time of this outbreak – it’s tricky to know what to do with this information from an infection prevention and control viewpoint!
This study illustrates the subtle complexity that goes with investigating an outbreak caused by an unusual carbapenemase across multiple species and hospital pathways. Without WGS we probably wouldn’t be having this conversation – so it’s a good thing that we are. But still some important unanswered questions remain around how far we can go in investigating and interrupting CPE plasmid spread.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
