If you pick an AMR bacterium of your choice, go to EARS-Net and plot prevalence across Europe, in most cases you’ll see a rough ‘north-south’ divide, with northern European countries doing better than southern European countries in terms of AMR rates (e.g. see below for antibiotic-resistant K. pneumoniae). What is driving this difference in AMR rates? A session at this year’s ECCMID asked just that question, hypothesising that weather / climate, economics, patient mix, or culture explain the difference. It was a fascinating session, so I thought I’d share some highlights!
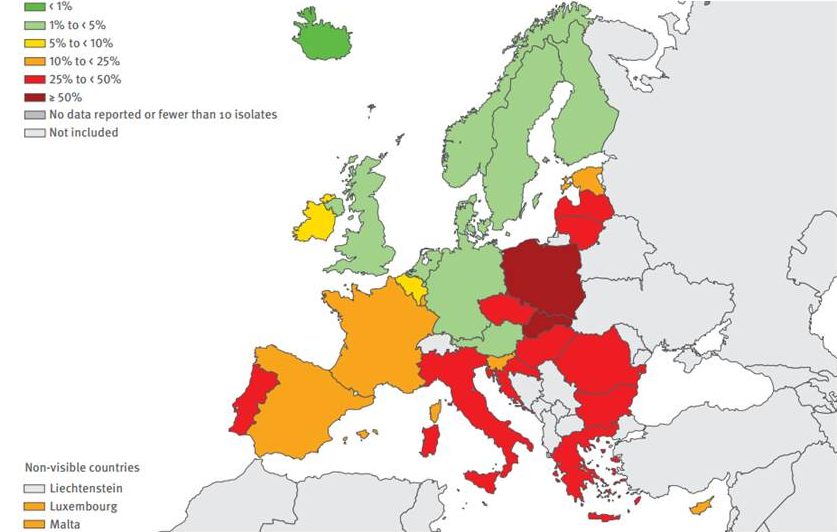
Figure 1: Klebsiella pneumoniae. % of invasive isolates with combined resistance to fluoroquinolones, third-generation cephalosporins, and aminoglycosides, by country, EU/EEA countries, 2015, EARS-Net.
Before I get to the details, a quick disclaimer: I have been criticised recently for seeming to defame entire countries by highlighting national AMR rates. So, worth clarifying that within a country with a high rate of AMR, there will indeed be individual hospitals and regions that have a very low rate of AMR. It’s worth reflecting on how a country gets to a high AMR rate. In many cases, I suspect the progression is first an individual hospital sees high rates locally, then, if unchecked, this spreads regionally, and finally, nationally. So, to be clear, I am not trying to cast aspersions on the infection prevention practice in any country – I know that my colleagues around the world are doing everything they can to prevent the spread of AMR (and other) organisms.
And so to the ECCMID session…
Weather / climate (David Fisman)
It is know that seasonal variation in ID occurs. There are striking summertime peaks of pink (Gram-neg) but not purple (Gram-pos) infections, latitude is associated with GNBSI, and the El Niño Southern Oscillation drives ID hospitalisation in the US. However, co-correlated environmental variables make it difficult to know why: temperature, pollen, ice cream sales… An interesting hypothesis is that more energy in the microbial ecosystem in the warmer summertime months accelerates horizontal gene transfer, and there’s some supporting lab data for this idea. But the mechanism for summertime peaks in some ID/AMR troubles remains largely elusive. (As an aside, David introduced me to Resistance Open, a seriously cool web trawler for AMR data.)
Economics (Ramanan Laxminarayan)
Some recent articles (here and here) in The Economist set the scene for the link between AMR and the economy. Much of the talk focussed on the antibiotic use, which is a fair proxy for national AMR rates I think! Antibiotic consumption increases with GDP, although usage in countries with lower GDP like India is skyrocketing. China is a huge user of antibiotics, consuming more than the top 10 countries combined. Perhaps unsurprisingly, there’s a huge burden of AMR in China. Some of the economics around antibiotic usage is just plain wrong. When hospitals are financially incentivised for prescribing antibiotics, antibiotic use will rise. Also worth noting that the price of antibiotics influences prescribers, to a larger extent than a prescriber would self-report, no doubt! Surprisingly, the economic cost of withdrawing antibiotic growth promoters in livestock is surprisingly small, and yet the ecological benefit is huge. Finally, to sum it up: “the rich pay with their wallet, the poor pay with their lives”.
Patient mix (Evelina Tacconelli)
Evelina Tacconelli produced a masterpiece, pulling patient demographic data from Eurostat to see what correlated with high or low AMR rates. I wish that I had taken far more comprehensive notes (was too busy listening!) but the bottom line was that some patient demographics seemed to correlate fairly well with AMR rates (from memory – diabetes, indices of deprivation) whereas others did not (again, from memory, age, length of hospital stay). No single demographic factor was a perfect match though. I hope that Evelina decides to turn the talk into a paper!
Culture (Peter Collignon)
This was in many ways the most interesting but also the most uncomfortable talk, suggesting that cultural factors may have a major influence on AMR rates. A World Bank report on AMR calls for better ‘governance’ of antibiotic use, which is an interesting idea. Much of the talk focussed on the link between corruption and AMR. Why is it that countries with more corruption have higher rates of AMR? Is corruption itself directly linked with AMR (e.g. through poor quality and counterfeit antibiotics), or is corruption a marker of other things that drive AMR (e.g. a ‘rule-breaking’ society)?
Summary
I have blogged before about how all sorts of variables co-correlate with MRSA rates in Europe: national debt, IPCN/ICD staffing, and antibiotic usage use. I think the one factor that weaves the variables together is socioeconomic status. Socieconomic status itself is a complex conundrum, with multiple co-correlated variables (education, income, housing, access to healthcare, diet to name but a few). Socioeconomic status is a patient-level risk factor that is associated with antibiotic usage, and rates of AMR bacteria. A high frequency of individuals with low socioeconomic status is also a marker of a failing economy, and society beginning to fray. It is easy to see how AMR bacteria would thrive in this environment: governments frankly have bigger fish to fry than focussing on AMR bacteria; healthcare systems are poorly funded and, like governments, focus their attention on immediate needs (like stopping patients from expiring there and then) rather than more strategic objectives like reducing AMR rates. So the answer to this is simple: if you want to reduce rates of AMR bacteria, we just need to stamp out low socioeconomic status.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

As an addition, I really like this article, which describes how corruption and poor governance is better correlated with AMR than volumes of antibiotic use. https://www.ncbi.nlm.nih.gov/pubmed/25786027
Gives to think. In the end it all ties together: you need a good medical infrastructure, we need patients to trust doctors, doctors need to trust the government, and a government needs to be reliable and provide a solid backbone for healthcare. We can’t expect a state that is dysfunctional on a fundamental level to take part in solving such a complex problem.
LikeLike