Great to see another fantastic annual ESPAUR report. It really is marvellous to have such a clear picture of HCAI and AMR related trends. As ever, there is some good news and some not so good news. Here three key headlines:
- Trends in bloodstream infection, antimicrobial resistance, and antimicrobial prescribing have changed during the pandemic.
- Tackling deprivation is tackling HCAI and AMR.
- We need to keep an eye on CPE
Trends in serious infection, antimicrobial resistance, and antimicrobial prescribing have changed during the pandemic
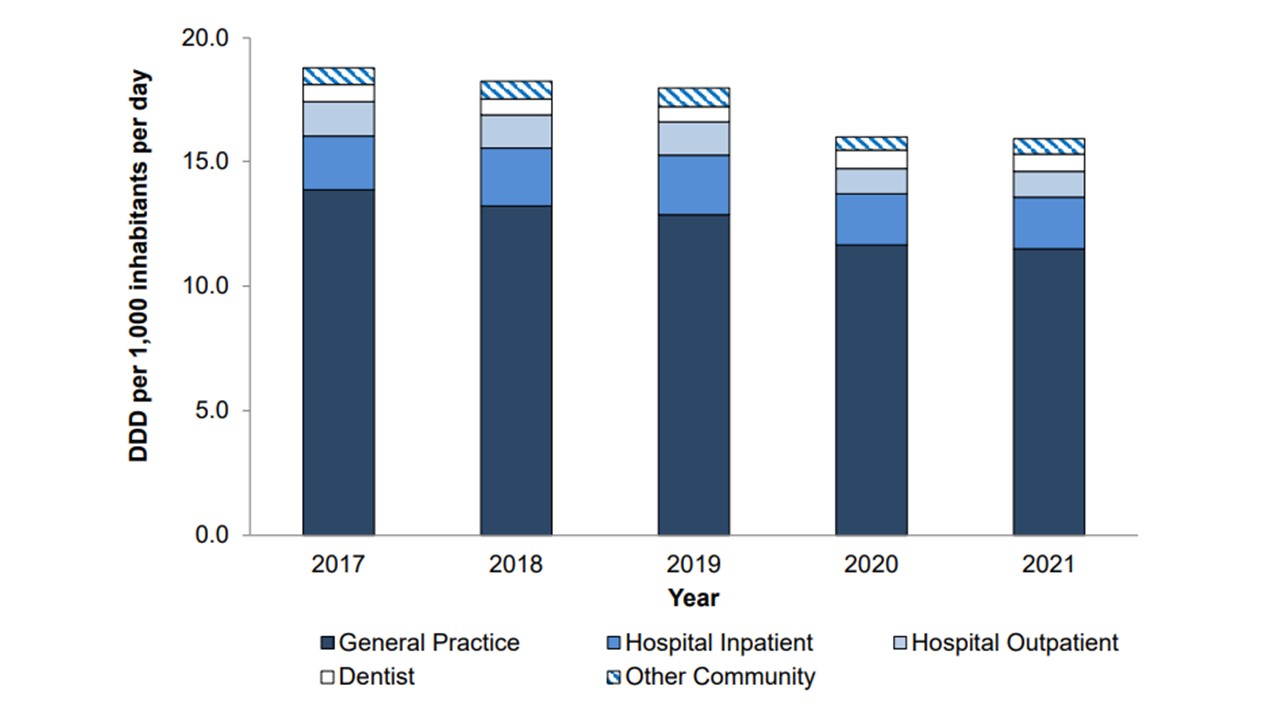
Perhaps unsurprisingly, turning our healthcare system upside down and giving it a good shake during the pandemic has resulted in some changes in trends of bloodstream infection, antimicrobial resistance, and antimicrobial prescribing. E. coli and Streptococcus pneumoniae BSIs were considerably less common on a population level during 2020 and 2021, bucking the year-on-year increase in previous years (Fig 1). This was not true for other key pathogens. Another apparently beneficial trend linked to the pandemic is a reduction in overall antibiotic-resistant bloodstream infections, and a similar trend in overall antibiotic consumption (Fig 2 and 3). This doesn’t bring out some of the more subtle trends associated with the pandemic, not least the peaks in prescribing driven by waves of respiratory infection arriving in hospital.
Figure 1. Annual incidence rate of key pathogen BSI, per 100,000 population, England 2017 to 2021 Note in this graph, the asterisk denotes that Escherichia coli and Staphylococcus aureus incidence is based on mandatory surveillance data.

Figure 2. Annual estimated total of (the burden) of antibiotic-resistant bloodstream episodes, England 2017 to 2021.

Figure 3. Total antibiotic consumption by setting, expressed as DDDs per 1,000 inhabitants per day, England, 2017 to 2021.
Tackling deprivation is tackling HCAI and AMR
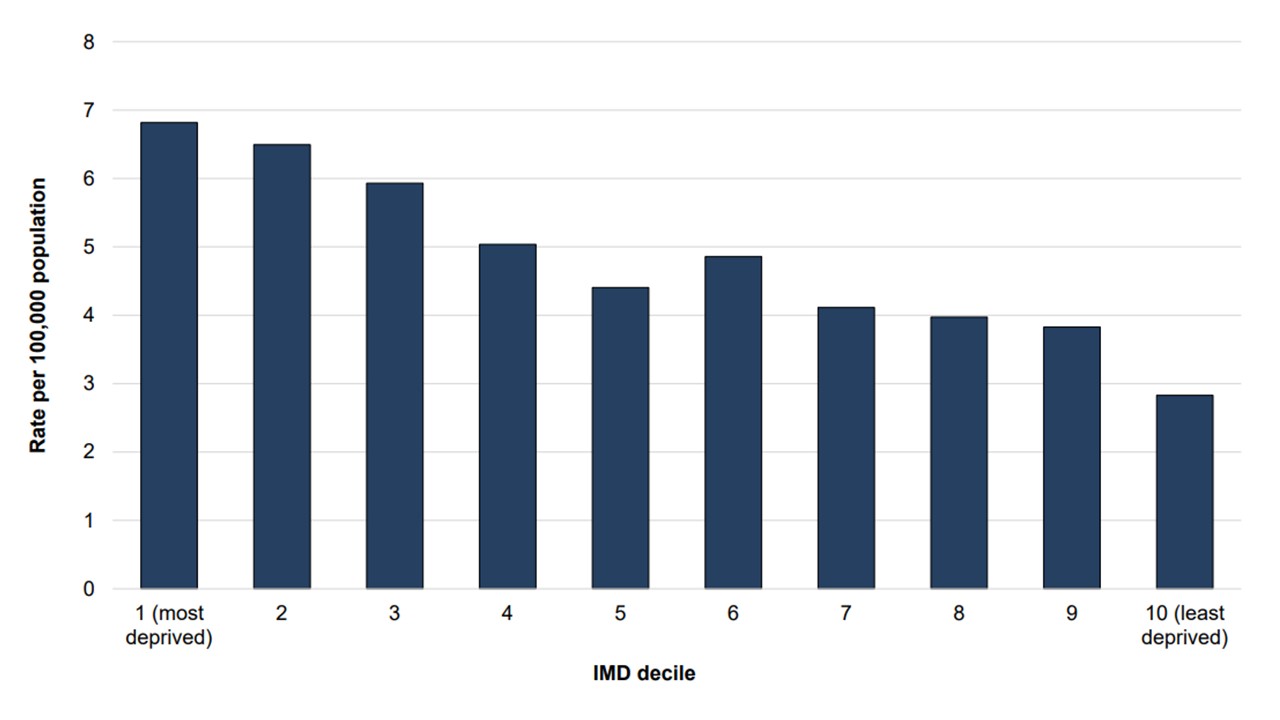
One of the most striking aspects of the report is the tight link between deprivation, infection, and antimicrobial resistance. As has been shown in many other areas of infectious diseases, social and material deprivation are key drivers for infection and antimicrobial resistance. The reasons behind this are multifactorial, but include overall health, health literacy, and access to healthcare. In this latest ESPAUR report, this comes out in at least two ways. Firstly the burden of AMR in BSIs varies by ethnic group in England, with resistance in the ‘Black, African, Caribbean, or Black British’ and ‘Any other’ ethnic groups about 10 or 11 percentage points higher than the 21% in those in the ‘White’ ethnic group (Table 1). Also, the rate of CPE per 100,000 population is more than double for those in the top Index of Multiple Deprivation (IMD) decile (almost 7 per 100,000) compared with the top (least deprived) decile (less than 3 per 100,000) (Figure 4).
Table 1. AMR burden from BSI by ethnic group in England in 2021. For this table, 598 (1.0%) BSI episodes could not be linked to obtain ethnic group information. The percentage resistant in this group was 21.6% (n=129; no ascertainment factor adjustment used).

Figure 4. Rate of acquired carbapenemase-producing Gram-negative bacteria notifications per 100,000 population by IMD decile in England, 2021.
We need to keep an eye on CPE
I think it’s fair to say we have diluted our capacity to respond to emerging AMR issues by focussing some much activity on the management of the pandemic, and rightly so. However, as the pandemic fades into history, it’s time to refocus our attention on emerging AMR issues, illustrated by the rise of CPE. The pattern of notification of CPE to UKHSA has changed, and is no longer encouraged – so there’s certainly some reporting bias in these figures. There does seem to be a clear regional difference in the prevalence of the “big-5” carbapenemases (Fig 5). What’s behind this difference? Could it be true that different regions of the UK are somehow a better ecological niche for a given carbapenemase? Or is it rather (as I suspect) that time and change has meant that a particular clone (bearing its particular carbapenemase) has become established in one geographical location?
Figure 5. Regional notifications per 100,000 population of acquired carbapenemase-producing Gram-negative bacteria by big-5 carbapenemase in England, 2021.

There’s much to digest in the report – but I hope it will serve as a reminder to us all not to lose our focus on issues related to antimicrobial resistance as this year’s world antibiotic awareness week draws to a close.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

“The pattern of notification of CPE to UKHSA has changed, and is no longer encouraged – so there’s certainly some reporting bias in these figures. ”
It’s correct that referral of all locally-confirmed CPE to the AMRHAI Reference Unit is no longer encouraged unless isolates originate from an invasive infection. However, acquired carbapenemase-producing Gram-negatives have been notifiable to UKHSA since October 2020.
https://www.gov.uk/guidance/notifiable-diseases-and-causative-organisms-how-to-report
LikeLike
Thanks Katie incredibly helpful comment
LikeLike