We talk often about the 5 Moments for Hand Hygiene but frequently neglect the 5th moment (after contact with a patient’s environment). So much so, that you might even describe this as the “Cinderella moment for hand hygiene”! Could it be that the Cinderella moment is actually the most important in the transmission of pathogens that cause HCAI? Maybe sometimes. But that’s missing the point. If we don’t focus our attention on all moments for hand hygiene, we won’t be as effective as we could be in preventing cross-transmission.
The routes of transmission for pathogens that cause HCAI are complicated and difficult to disentangle. Just take all the controversy about exactly how the air is a vector in the transmission of SARS-CoV-2! But that’s not the only controversy in HCAI transmission routes. For a long time, people questioned whether environmental surface contamination played any significant role in the transmission of pathogens that cause HCAI. I hope that this particular controversy has been firmly put to bed now: we have mountains of evidence that environmental surface contamination plays a pivotal role in the transmission of many pathogens that cause can cause HCAI most of the time. However, what is the relative importance of hand contamination vs. surface contamination?
I gave a talk today at the inaugural “Environment, Cleaning, and Decontamination (ECD)” conference about exactly this question. (You can download my slides here.) I made the case that we have really good evidence that both hand contamination and surface contamination are independently important in the transmission of pathogens that cause HCAI. Fundamentally, there is a dynamic and fluid interplay between hand and surface contamination. So much so, that it’s quite difficult to disentangle the relative importance of each; in a sense, hands are just another high touch surface that is often contaminated and rarely disinfected! It’s no surprise, then, that the chances of picking up an MDRO on your hands are approximately equal if you touch the ‘surface’ of a patient who is colonised with an MDRO compared with an inanimate surface in their immediate environment. Also, probably because there is less of a psychological trigger, compliance with hand hygiene following contact with the environment (“the thorny 5th moment”) is lower than following direct patient contact (reinforced by this excellent modelling study). So, could it be that contamination acquired on hands following contact with environmental surfaces is relatively more risky than contamination acquired through direct patient contact because the probability of hand hygiene is lower?
The dynamic interplay between hand and surface contamination is illustrated vividly and, I think, rather beautifully by the classic ‘Oelberg’ study. In this study, a cauliflower DNA marker was inoculated onto a telephone receiver in part of a neonatal ICU. Within hours, the marker had spread to the hands of every single healthcare worker present in that part of the ICU, and simultaneously onto a high proportion of inanimate surfaces. Clearly, this wasn’t a whole micro-organism so may not reflect exactly how a real organism would spread. But it’s really powerful proof of concept.
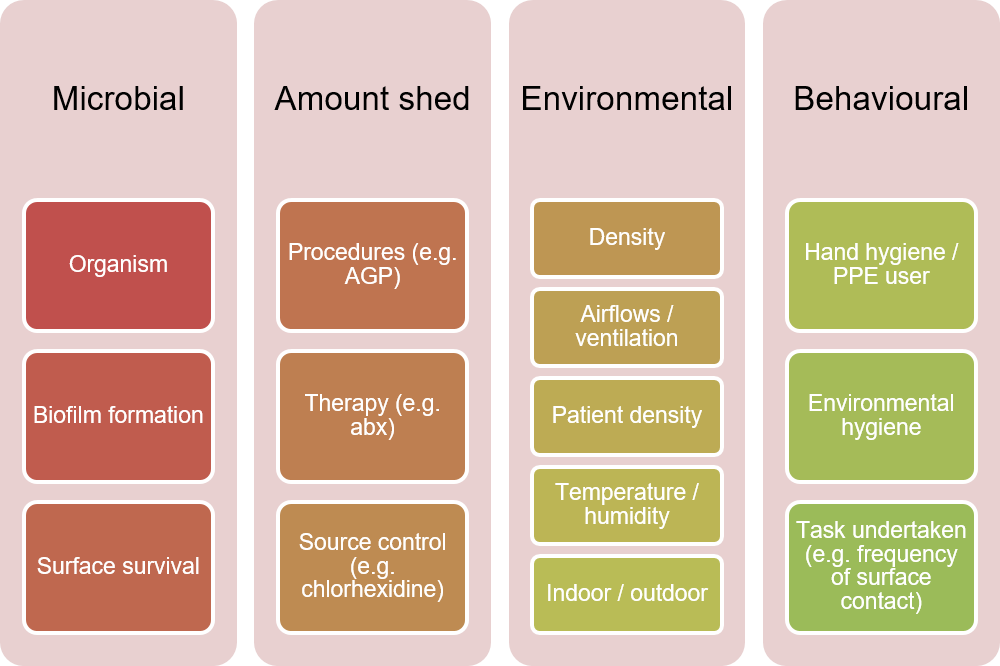
I think the best way to try to disentangle the relative importance of hand and surface contamination is through mathematical modelling. (Yes, ‘all models are wrong but some are useful’!) For example, one model examined the transmission of three common viruses: Influenza, Norovirus, and Rhinovirus. The model was parameterised to estimate the overall basic reproduction number (R0), the R value of fomite-mediated transmission, and the R value of fomite+hand mediated transmission. As you would expect, Norovirus was most driven by fomite-mediated transmission, whereas this was more influenced by circumstance for Influenza. Thinking about it, there are quite a few factors, themselves inter-linked, that will influence the relative importance of hands and surfaces in transmission (see Figure 1).
So where does all this leave us? Hand hygiene and surface hygiene are both independently important in reducing the transmission of pathogens that cause HCAI. There is a dynamic interplay between the two, making it really hard to disentangle the relative impact of either route. Here, we turn to modelling again to examine the comparative effectiveness of hand vs. surface hygiene interventions. For example, one study showed that in the context of C. difficile transmission in an inpatient setting, increasing the frequently of surface hygiene had more of an impact than increasing the frequency of hand hygiene. However, this picture will change with pathogen and circumstance. Perhaps the most important outcome of the model is that the rate of infection dropped to its lowest when hand and surface hygiene interventions were combined. Therefore, due to the collision of hands and surfaces in the transmission of HCAI, we must focus on improving both hand and surface hygiene to maximise patient safety.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

Very nice slide deck! Thanks for your generosity in sharing
LikeLike
Thanks – all my slides here: https://jonotter.net/
LikeLike