I gave a talk at the Sussex Infection Prevention Development Week yesterday on ventilation and preventing the spread of SARS-CoV-2. I learnt a lot in putting together the talk, so thought I’d share my slides (here) and some of the key points. Ventilation is a crucial way to prevent the spread of SARS-CoV-2 (and other respiratory viruses), and I hope that improved ventilation in health and social care settings will be one of the good things to come out of this pandemic.
Transmission routes
Respiratory viruses are versatile beasts, able to spread by all of the key transmission routes under some circumstances: contact (including indirect contact spread via surfaces), droplet, and airborne routes. This is true of influenza, SARS-CoV-1, SARS-CoV-2 and many others. I wrote a review paper in 2016 reviewing the evidence for the role of contaminated surfaces in the transmission of respiratory viruses. The image below is from that review (dated 2016). I think it’s still helpful to illustrate the various transmission routes for respiratory viruses, but the definitions of “droplets” and “droplet nuclei” now seem rather dated.
Knowing that respiratory have the capacity to spread by these routes under some circumstances is the easy part – knowing which route is predominant under a given set of circumstances is much more challenging. We need to pull together the full range of scientific discovery methods to get to the bottom of this (lab studies, clinical epidemiology, mathematical modelling, and perhaps a bit of philosophy!). And then there is a great deal of uncertainty even for a well-studied virus like influenza.
An important part of the discussion is how transmissible SARS-CoV-2 appears to be, as measured by things like secondary attack rate and basic reproductive number. The mean secondary attack rate for SARS-CoV-2 is about 20% to household members. That’s a little lower than you may expect. And the R0 is about 2.5-3, which is a little higher than for influenza but considerably lower than for measles. Just to be clear though, these are not measures of “airborneness” but rather measures of transmissibility by any and every route.
I found a recent opinion/review article in JHI helpful in pulling together some of the evidence around transmission routes for respiratory viruses involving air as a vector. The article set out to bust some common myths about airborne transmission of SARS-CoV-2. I found the arguments about particle size helpful. Historically, we have used a rather arbitrary “5µm” cut off for defining a droplet (>5µm) and an aerosol (<5µm). However, two important points here. Firstly, the particles that are expelled from the respiratory tract by speaking, singing, shouting and, indeed, just being alive are a continuum of particle sizes. And secondly, if we’re going to have an arbitrary cut-off for the particles that are likely to fall within 1-2m of the source most of the time, 100µm would be more like it. The other part of the article that I found helpful was the description of the way that masks work. One the face of it, a surgical mask (or indeed a HEPA filter) is too porous to catch a SARS-CoV-2 virion because the holes are too big. But filters that aim to remove particles (be it dust or a virus) from an airstream don’t work like a sieve. There are some interesting physical forces at play meaning that the various layers of the filter material are able to capture a much smaller particle than you may expect. And therefore, the efficacy of any type of mask is not binary but rather a risk reduction exercise.
Controversy and uncertainty about transmission routes of respiratory viruses is not new (remember the classic “It’s airborne” line from the 1995 classic Outbreak?).
What do the public health agencies say about transmission routes for SARS-CoV-2?
Despite the well-documented differences in recommendations from WHO, PHE, and CDC, all three bodies have a very similar description of the transmission routes and dynamics of the SARS-CoV-2 virus (WHO, CDC, PHE). To paraphrase:
- SARS-CoV-2 can be spread by respiratory particles (droplet and airborne routes) and through contact.
- The predominant route is through prolonged close proximity.
- Airborne transmission of SARS-CoV-2 can occur under special circumstances, especially in enclosed spaces.
- Transmission via the contact route is less common.
- There remains considerable uncertainty over transmission routes.
PPE
PPE has been one of the most charged aspects of the pandemic, with CDC recommending FFP respirators (N95 equivalent) for healthcare workers caring for patients with confirmed or suspected COVID-19 vs. WHO and PHE recommending surgical masks when caring for these patients except when possibly exposed to aerosol generating procedures, in which case an FFP respirator should be used.
We could talk until the bats come home (see what I did there) about this. But one thing is without doubt in this space: overuse and misuse of PPE can result in more risk to the wearer (through self-inoculation) and increased risks of cross-transmission. So, whatever PPE is recommended nationally and locally where you are working, it is vital to support staff to use PPE safely and effectively. We developed an on-the-ground support programme of “PPE Helpers”, which I hope led to some important improvements in the safe and effective use of PPE.
Engineering controls
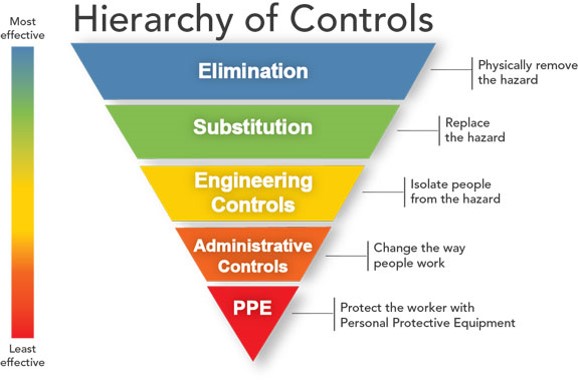
The hierarchy of controls to reduce a risk have PPE right at the bottom of the pyramid, as the least effective way of managing a risk. Engineering controls (like improving ventilation) are higher up the pyramid and as such more desirable.
There’s some great evidence that improving natural ventilation through, for example, opening windows, can have a large effect on improving ventilation and reducing transmission risk. A review paper summarises neatly the various approaches that can be taken to improving ventilation. Drawing from this and a helpful SAGE report on the same topic, I cobbled together the table below, which I hope provides some practical steps that can be taken to improve ventilation in health and social care settings.
| Measure | Considerations |
| Get to know your ventilation systems | Natural, mechanical, specialist – and read the relevant HTM 03-01. |
| Increased use of natural ventilation (e.g. opening window and door) | Relies on human behaviour; temperature issues; potential safety/security issues; temporary changes less effective but mitigates some of these risks. |
| Find ways to get more out of existing HVAC systems | Increase fresh air, reduce recircualation, extend operation; requires input from Estates; may disrupt airflows; may require qualification testing. |
| Installation of new passive (louvres/air bricks) or mechanical (extract fans, new HVAC) systems | Requires input from Estates; may be costly; may disrupt airflows. |
| Breaks or fallow periods between occupants | May interrupt patient or staff flow in an area. |
| Use of local air filtration / disinfection devices | Lack of evidence of clinical impact; may be useful in enclosed indoor spaces, |
Innovation
With many unknowns about the relative contribution of the various transmission routes, and around the best way to address them, there big opportunity for applied research in this space. Several different technologies are around that may help us to improve ventilation and/or the management of patients to reduce the risk of spreading respiratory viruses in the air. For example:
- A range of stand-alone air disinfection / filtration devices are on the market, which have shown impressive results in improving indoor air quality. However, evidence of clinical impact is not quite there.
- I have seen a number of variations on the theme of a ‘tent’ that goes over a patients top half to capture aerosols produced during certain procedures (I hope you appreciate this very technical description). A promising approach, with further findings anticipated.
- The use of temporary single rooms to either contain patients with possible or confirmed respiratory viruses, or to free-up single room bedstock to do this more effectively. Some evidence that this approach is effective in a PICU setting here.
Beyond COVID-19
The issues raised by SARS-CoV-2 around transmission routes, the role and importance of ventilation, and the need for good multidisciplinary science stretch far beyond COVID-19. The air is known to harbour a range of pathogens in hospitals – and not just respiratory viruses. We know that MRSA, C. difficile spores and other organisms can be cultured from hospital air. So, I hope that the raised profile of the importance of good ventilation in the prevention of infectious diseases will continue well beyond this pandemic era.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

Thanks for sharing
LikeLike
Super helpful as always! Thanks.
LikeLike
https://doi.org/10.1101/2021.04.27.441510
USAMRIID has demonstrated on non-human primates that aerosols give more serious disease than intra nasal or tracheal inoculation. Why are CDC US and ECDC and WHO denying the danger? Droplet short range ideas protects IATA but kill people!
LikeLike
Hi CDC, ECDC, WHO, and PHE all acknowledge airborne transmission of SARS-CoV-2 under some circumstances.
LikeLike