Today, the Journal of Hospital Infection have published an article from our research group about E. coli BSI sources. The key message is that the sources of E. coli BSIs at a large teaching hospital differ considerably from the national average, with a large proportion related to febrile neutropaenia (18%) and diverse gastrointestinal sources (15%). This calls into question the ‘preventable’ proportion of these cases – and adds something to the discussion as to whether the national ambition to halve GNBSI by 2021 is feasible.
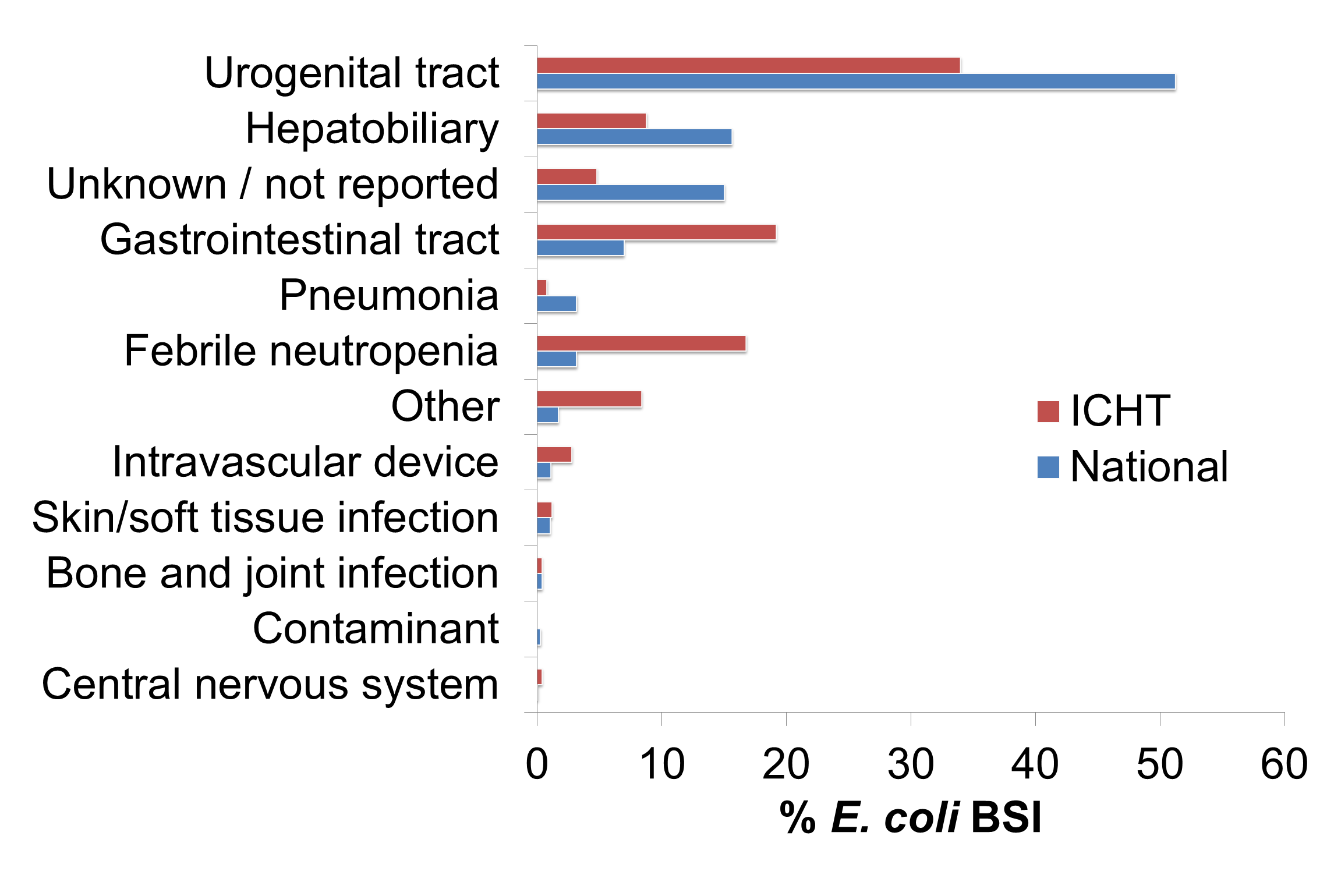
We reviewed in detail the 250 cases of healthcare-associated E. coli BSI between the 2014/15 and 2016/17 financial years. The sources of the cases is summarised in the Figure. As you can see, the local picture differs considerably from the national picture. Whilst urinary sources are common, they are not as common as in the national picture. Also, febrile neutropaenia (18%) and gastrointestinal sources (15%) were considerably more common than in the national study. Cases were rarely associated with surgical procedures (4%) or indwelling vascular devices (3%).
Figure: E. coli BSI sources nationally vs. locally. Note: the national dataset includes community-associated and hospital-associated cases, whereas the local dataset includes only hospital-associated cases.
We performed some regression analysis to examine whether any risk factors for a particular source stood out. Female gender (odds ratio 2.3, 95% confidence interval 1.2-4.6) and older age (OR 1.02, CI 1.00-1.05) were significantly associated with a urinary source, but there were no significant associations identified with gastrointestinal source BSI or febrile neutropaenia related BSIs. Also, we found that the levels of antibiotic resistance were higher in our isolates than the national average, which isn’t too surprising given the differences in patient mix.
We observed an increase in the total number of cases, rising about 25% over the study period in line with national trends. However, whereas the number and rate of blood cultures tested by the lab has risen in proportion to the number of E. coli BSIs detected, the proportion of positive blood cultures that were E. coli BSIs did not change over the study period. Also, the number of patients admitted (a measure of activity) has increased over the study. This suggests that the increase in detection of E. coli BSIs isn’t a relative increase in E. coli compared with other causes of BSI, but a combination of an increased throughput of patients combined with improved awareness around the need to take blood cultures when investigating patients who may have sepsis.
So where does this leave us in trying to halve GNBSIs by 2021? The pathogenesis of some gastrointestinal E. coli BSIs and most BSIs associated with febrile neutropaenia is likely to result from translocation of endogenous bacteria to usually sterile tissues as a complication of other interventions. Therefore, E. coli BSIs that are associated with febrile neutropaeia or gastrointestinal sources are likely to be less preventable than other sources – and in our setting, this was one third of the cases! However, there are still substantial opportunities for E. coli BSI reduction in, for example, cases with a urinary source – and especially a urinary catheter source. In last year’s ‘Can we halve GNBSIs?’ debate with Martin, I argued that we can halve GNSBI – and I still think that this is true…but I’m not sure that this is true in every setting!
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
