Earlier this year, CMI published our article on the cost of a CPE outbreak in London, which cost 1.1m (Euros) over 10 months. EID have recently published a similar article, reporting a 0.6m (Euro) outbreak of CPE in the Netherlands.
The outbreak of NDM-producing K. pneumoniae occurred over 4 months in 2015, and included 29 patients. This was a typically Dutch ‘search and destroy’ approach to outbreak management: the discovery of a few epidemiologically-related cases on a surgical ward triggered screening of all inpatients in the 700 bed hospital! This identified 7 wards with 2 or more NDM carriers. A phenomenal 95% of the ~3000 patients identified as being ‘at risk’ (having spent time on one of the wards) were screened over the next 6 months. Interestingly, no risk factors (such as overseas travel) were identified in the 29 case patients (which is similar to our experience during the 2015 K. pneumoniae NDM outbreak). This suggests to me that a single undetected introduction of the outbreak strain was followed by horizontal spread within the hospital.
Figure 1: Counting the cost of the Dutch CPE outbreak (with my designation of actual expenditure and opportunity cost, not the authors’!)
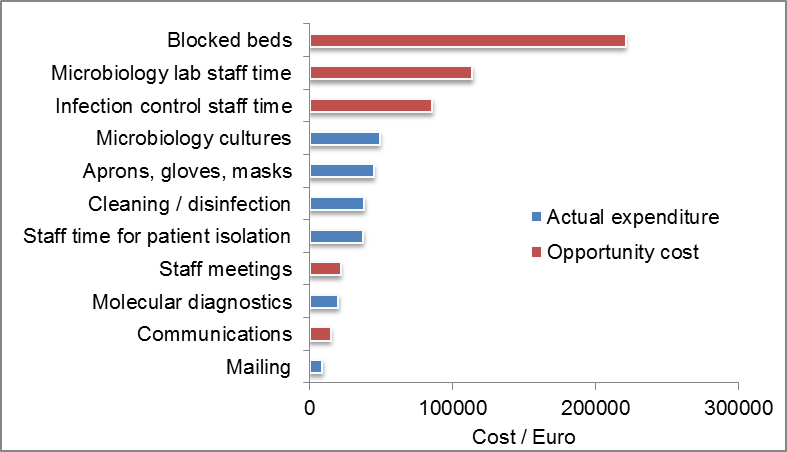
The team took a similar approach to counting the cost of the outbreak to us, listing everything that was done and adding a price tag to each line. The bottom line was a 0.6m Euro price tag over four months, accounting for 12% of the hospitals budget for clinical microbiology and infection control! The cost of around 23k Euro per patient was similar to ours (27k Euro per patient). A few discussion points:
- I would have liked to have seen more distinction between the actual expenditure incurred (e.g. extra spend on lab reagents) and opportunity cost (e.g. staff time which is a fixed cost, but redeployed to managing the outbreak in place of other activities). By my count, actual expenditure was around 200k Euros and opportunity cost was 460k Euros (see Figure 1).
- There was no information or costs on the treatment of patient who developed infections.
- The large cost of blocked beds is an interesting one. Presumably these beds were blocked due to actual bed closures resulting from infection control management of the situation rather than extended length of stay of the case patients. In our evaluation, we included both the cost of additional length of stay of the case patients (adjusted for time to event) and the cost of beds blocked due to infection control management.
- Since the outbreak centred (or at least was first identified) in a surgical ward, I wonder whether any procedures were cancelled as a result? This was the largest single cost in our evaluation.
- I was surprised not to see reference to the CHEERS guidelines, which are designed to promote consistency in the way that economic evaluations are performed and reported.
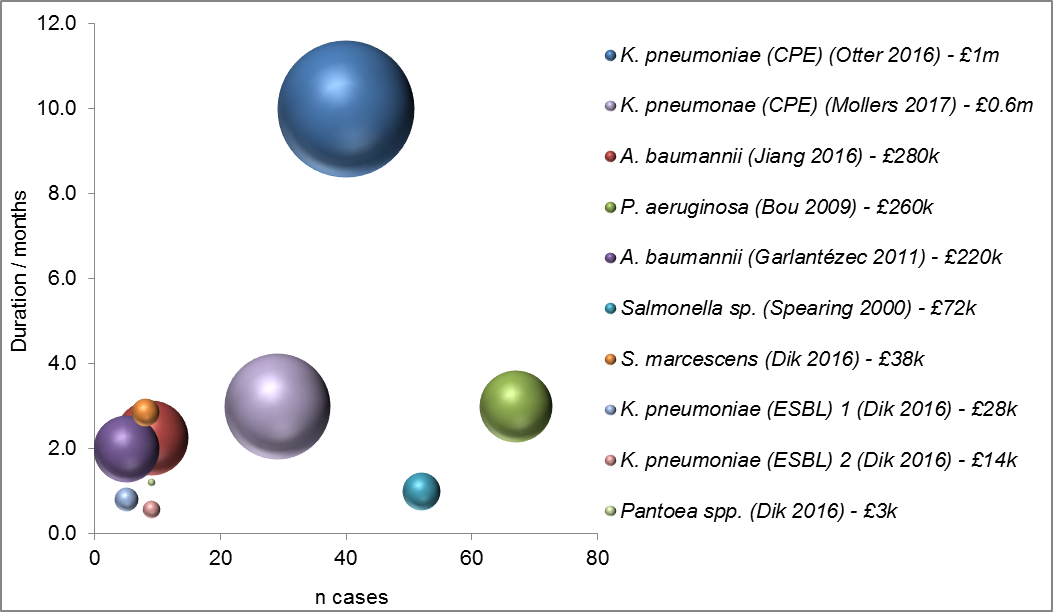
Figure 2: Summary of studies evaluating the cost of outbreaks due to Gram-negative bacteria in hospitals. The cost of the outbreak is represented by the size of the bubble (aka the z axis).
Overall a helpful study which reinforces that even small outbreaks of antibiotic-resistant Gram-negative bacteria result in substantial costs to an organisation. I get the feeling that if the hospital hadn’t taken the measures that they did, they would be staring down the barrel of an endemic CPE problem (remember the 29 patients were spread over 7 wards in the hospital). Clearly, this argues for upfront investment in strong prevention activities rather than larger but later splurging of cash to control a problem after the horse has bolted!
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.

Indeed interesting, but I do have some questions on the methodology. The laudated Dutch approach is effective, but also very extensive (multiple measures implemented at the same time). Yet, the (relative) effectiveness of each of these measures is unknown. So yes, closing beds costs a lot, but it is unknown whether it was necessary to make these costs. The next 2 cost drivers were staff time for infection control and microbiology. Yet, these people were already employed and controlling an outbreak and laboratory work their job, I presume. So, without the outbreak the personel costs for the hospital would have been the same. Unless additional staff was hired, which was not described. So, I think an outbreak is expensive, but not as expensive as this, and effective controlling could have been less expensive.
LikeLike
Hi Marc yes important to understand the difference between actual expenditure and opportunity cost. Staff time is a pretty soft opportunity cost: these are fixed costs that are not changed by having an outbreak – they just mean that staff are focused on one thing and not another. There are other categories of opportunity cost that are more ‘real’ e.g. missed revenue from elective surgical procedures. Whilst the outbreak does not result in increased expenditure, it does affect the hospital’s balance sheet due to reduced revenue (unlike staffing costs). As to whether bed closures reduce transmission, your guess is as good as mine. Perhaps a pragmatic cluster RCT would help? One hospital / ward / cluster implements early bed closures, another doesn’t!
LikeLike