The UK government has recently announced their ambition to halve the rate of Gram-negative BSIs by 2021. Looking at the latest mandatory reporting dataset (see Figure 1 below), you can see why. Impressive reductions in MRSA BSI and C. difficile, but a notable increase in E. coli BSI. And this combined this with worrying data around increased antimicrobial resistance in Gram-negative bacteria from the ESPAUR report. In this post, Martin Kiernan and Jon Otter present both sides of the argument as to whether Gram-negative BSIs can be reduced by 2021, with comment from Andreas Voss and Marc Bonten! And you get to vote on which side of the argument you come down on after reading the arguments. Let battle commence…
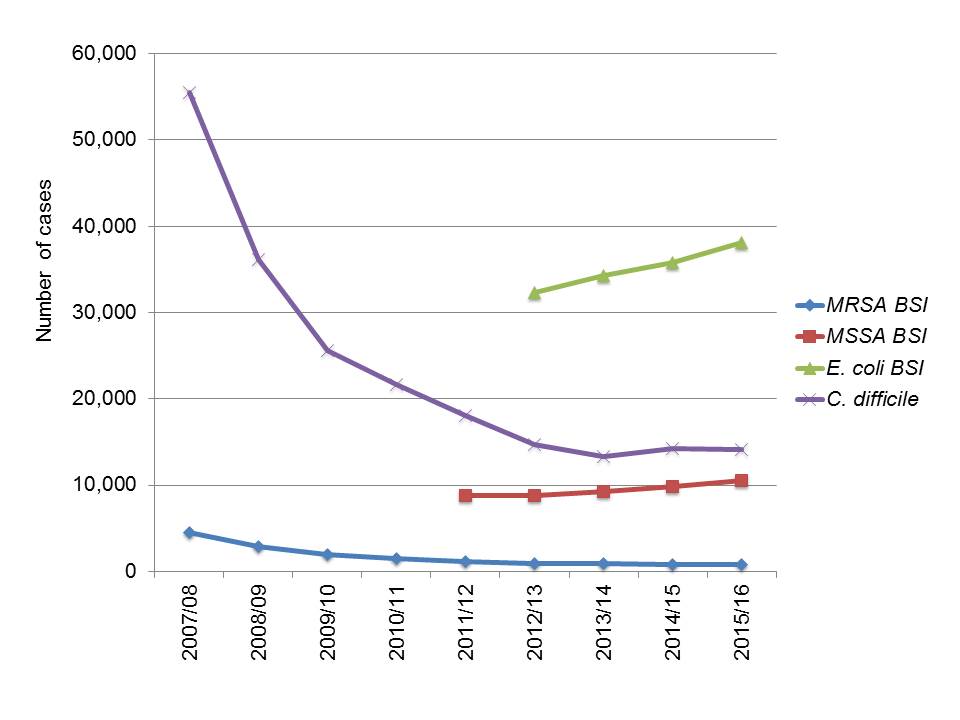
Figure 1: Trends in mandatory reporting data in England, 2007/8 – 2015/16.
NO WE CAN’T (Martin)
Jon had thrown down the gauntlet and I must accept for a chance of revenge following my defeat in last year’s CDI debate. He is of the opinion that a 50% reduction in Gram-negative BSIs is possible by 2021. I think that it is unlikely and I’ll outline my reasoning. For starters however I have to say that a national objective for England is a very good thing. It worked for MRSA and C. difficile through focusing minds on the problem. I’m unconvinced by the ‘it was all antibiotics all along’ argument recently espoused and feel that the focus on interventions with an evidence base (get the lines out asap, topical suppression for those with positive MRSA swabs, isolation, cleaning, etc etc) all contributed, as did hospitals looking at their own data, personalising cases in terms of root cause analyses and to some extent financial penalties.
So we move on to the escalating issue of Gram-negative bacteraemia and it is an altogether different beast. For starters, we don’t have much of an idea as to what is causing this increase. The literature is rather sparse on this and a recent publication has described the findings of some sentinel surveillance. A number of points have to be made. For starters, many of these infections are not healthcare-associated in the older sense of the word, i.e., hospital-associated. The healthcare contacts in the majority of cases are in primary care, where sadly there is a somewhat variable infection prevention resource in England (putting it mildly).
A report to the then ARHAI committee (Antimicrobial Resistance and Healthcare-Associated Infections) that I chaired in 2015 concluded that a relatively small percentage of these infections are device-associated and that the majority of cases arose from repeat visits to General Practitioners in primary care with urinary tract infections. We made a number of recommendations. No 1 was that EPIC 3 should be implemented and this means using bladder scanners prior to catheterisation. Sadly EPIC 3 is not NICE Guidance and therefore does not automatically drop into organisational governance systems and is therefore potentially ignored. I don’t think that the regulator in England (the Care Quality Commission) has ever asked to see the risk assessment and implementation programme for EPIC3 (please correct me if I am wrong).
The second recommendation was for monitoring hydration status in the elderly, bearing in mind that the great majority of cases are in persons >75 years of age who are reluctant to drink and with potential cognitive issues. We will also need to take into account the issues of seasonality and how hydration can be promoted effectively during warmer weather (this does not mean ‘drink more’ messages). The elderly with continence issues are reluctant to drink for a number of reasons and the availability and price of pads is just one of them. Whipping catheters out and not putting them in sounds great however resource will need to be put into continence care. Effective barrier methods of protecting the skin are required however many are only available in hospitals and this could be a balloon that is squeezed resulting in an increase in moisture lesions and pressure damage (also increasing the risk of infection).
We also recommended ‘safety netting’ of all patients treated with antibiotics for UTIs, however who and how this could happen will need some co-ordination and co-operation across the healthcare economy and to be honest I have no idea who will do this. The bottom line for me is that Gram-negative bacteraemia is going to be far tougher than MRSA and C. difficile was. So at the moment I’m a pessimist, mainly because the killer interventions have yet to be discovered and the people who will implement them have yet to be identified. We walk up an escalator that is going in the opposite direction, with an increasingly elderly population with escalating levels of co-morbidities. I hope that Jon wins the debate in the long term however until real collaboration starts to happen across the country I’m going to say that this objective won’t be met.
YES WE CAN! (Jon)
When the MRSA reduction targets were announced in 2003 – yep, almost 15 years ago – the feeling in the infection community was “no way can we achieve this target”. And I have to say that when the ambition of the government to halve healthcare-associated GNBSIs was announced recently, my initial response was similar. However, having taken a look at the data that we have available at this stage (in preparing this talk), I am feeling much more positive about achieving the reduction in GNBSI, starting with E. coli. And here’s how…
Getting to the root of the problem
Whilst this may have escaped the attention of some, E. coli BSI is not the same as MRSA BSI or C. difficile infection. Therefore, you can’t simply look at the English MRSA or C. difficile ‘miracles’ and automatically assume that the same sort of reductions will be achieved with E. coli, and, more broadly, all GNBSI. It’s a different challenge. But the differences between the epidemiology of E. coli and MRSA BSI also give me hope that we have a lot to go for in reducing them.
For example, recent data suggests that around half of E. coli BSIs have a root cause in a urinary tract infection. How many of these are associated with catheters that were either not required in the first place, or have been in place for far too long? Around 10% are related to a gastrointestinal source. Is there more to do in reducing the chances of E. coli making its way from the gut to the bloodstream? Surgical infections are likely to be a major vehicle for this journey – and we can certainly do more to identify and prevent surgical infections! Finally, around 25% of E. coli BSIs have an unknown source – is this because the source is unknowable, or could we do more in identifying the source which may open up new avenues to prevention? I do accept that there isn’t a great deal more we can do in reducing risk from vascular access devices, so I don’t see that as especially fruitful hunting ground in reducing GNBSIs (aside from sustaining the gain).
Appropriate use of antibacterials
We have gone a long way with reducing the inappropriate use of antibacterial agents – as illustrated by the overall reduction in antibacterial use across the healthcare sector in the UK reported for the first time in the latest ESPAUR report. However, do patients always receive the right antibiotics for Gram-negative infections in hospital and community settings, matching the susceptibility of the organism involved, which could lead to a BSI if left unchecked? Some places will be doing better than others at implementing this. Also, if declines in antibacterial usage continue outside of hospitals, selective pressure for resistant strains will diminish, which ought to make treatment of Gram-negative hospital infections more straightforward, with better outcomes (and less BSIs).
How much E. coli is hospital-acquired?
The answer is that we have no idea. The assumption is that not much cross-transmission of E. coli happens and that most E. coli infections have an ultimately endogenous source. However, this was also the perception for MRSA BSIs initially in the eyes of many, which turned out not to be the case at all! I am not suggesting that we try to interrupt the spread of all E. coli through a targeted approach, but perhaps now is the time to think carefully about whether to increase our efforts in preventing the transmission of resistant E. coli. For example, should we be screening for carriage of ESBL-producing E. coli? I accept that not many hospitals will have the capacity to isolate carriers, but it would certainly help in putting them on the appropriate therapy should an infection develop, which may reduce the chances of developing a BSI.
Targets up the ante
I remember visiting a London hospital in the late 2000s and meeting a head of IPC in the hospital canteen. We had a brief, chance meeting with the CEO, who asked only one question: “How are our MRSA BSIs looking this month”? I don’t think they would have been asking that question before the targets were introduced! My point being that reduction targets are a useful way of focussing the efforts and resources of a healthcare organisation. Once E. coli BSI rates begin to be compared with peer organisations, this will help us seek out areas for rapid attention and improvement. The public availability of mandatory reporting data (including E. coli BSIs) via Fingertips will help to promote this sense of organisational accountability, which should ultimately help to reduce GNBSI (see Figure 2 below). And financial penalties will help to focus the organisational mind further, if they are forthcoming.
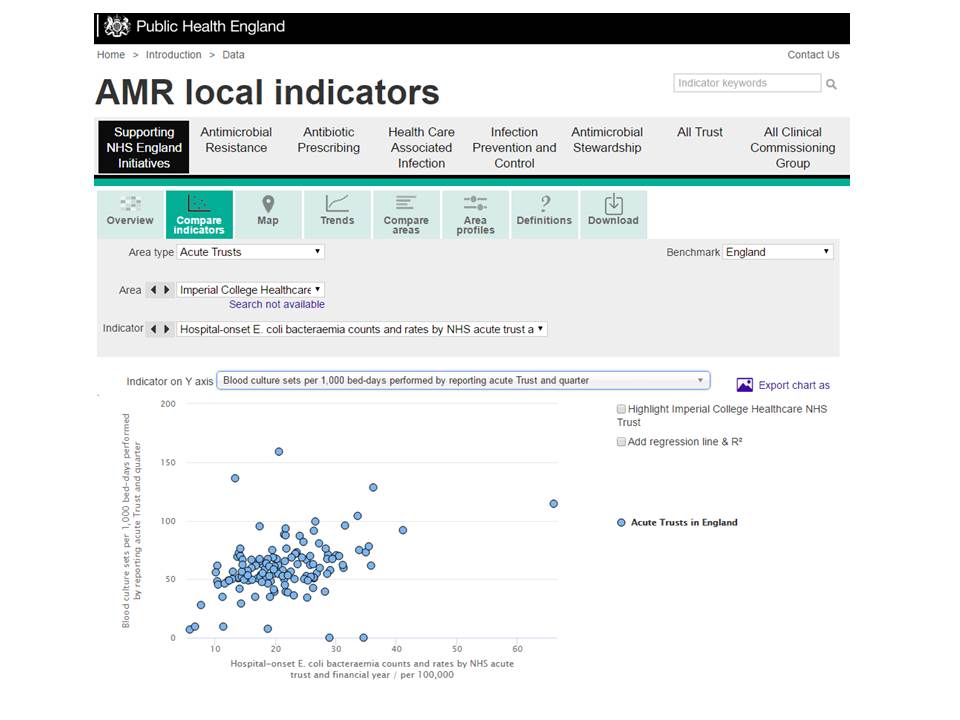
Figure 2: The rate of E. coli BSI plotted against the rate of blood culture sets (from PHE Fingertips).
Team working across the healthcare economy
Since most of us have E. coli as part of the normal gut flora, it is no surprise that community infections with E. coli are common – and some progress to BSIs. If we are to successfully tackle and reduce E. coli BSIs in hospitals, we need to be applying similar approaches in the community. It’s no good having tight protocols and procedures in hospitals if patients are not being managed and treated appropriately in the community, which would sometimes pre-dispose hospital-onset BSI. It is good to see a 10% reduction target for community-associated BSIs now in place.
Summary – yes we can!
There are some very important unknowns in deciding whether it is feasible to meet the target of halving GNBSIs by 2021. In the context of E. coli BSIs, what are the likely sources of these BSIs, and how many can be prevented without massive investment in personnel or technology (because I don’t see this investment coming our way any time soon). And then what about all the other Gram-negative BSIs? We know even less about the basic epidemiology of these serious infections. However, despite these uncertainties, I think we can be emboldened by the successes with MRSA BSI and C. difficile infection reductions and really go for halving GNBSIs by 2021. Even if we don’t reach the 50% reduction target, I feel certain that we can reverse the upward trend and in doing so improve the lives of our patients.
MODERATOR (Marc)
I am with Jon, although he probably won’t be with me. For me, the fundamental question is what proportion of E. coli BSI is preventable by what measure? We do know that the transmission rate – in the absence of effective control measures – of E. coli in hospital settings is lower than that of K. pneumoniae, MRSA and C. difficle. We also know that it took more than interrupting transmission to reduce MRSA (prevent line infection) and CDI (reduce antibiotic use). We also know (or at least think) that many if not most E. coli BSI originate from endogenous sources. So, the classic hospital-based infection control measures (hand hygiene, isolation, etc) won’t do much. So, I think if Jon states “Yes, we can”, he has the following three measures in mind:
- At least 50% reduction in obtaining blood cultures in patients with sepsis.
- Immunisation of all elderly with a highly effective coli conjugate vaccine.
- SDD, not only in ICU, but for all patients undergoing colo-rectal and gynaecological surgery.
If not, I am with Martin.
MODERATOR (Andreas)
The English have set a new goal to halve Gram-negative BSIs by 2021! No doubt that one can call this goal “ambitious” and going further than what the Dutch set as a goal for the same time-period: keeping the Netherlands CRE “free” (or at least no more than sporadic CRE infections). The question for you guys is, do you believe it is possible?
Let’s just mention the one point both agree on: a national objective to reduce Gram-negative BSIs is a noble and helpful one, and both recognize to a certain degree that – just as in games of chance – past results with MRSA and C. difficile is not a guarantee of future performances.
Jon and Martin asked for a pre- and post-survey commentary, but I will keep it to a “post-survey-comment” as I might otherwise add additional arguments to one side. I was tempted to add a third choice, namely “No the English can’t, but the Dutch might” but I believe that chances are – to a certain degree – the same in England and the Netherlands.
Time for you to read their arguments, and to look back into your own experience, before you cast your vote…
VOTE

At least 50% of E.coli BSI cases have a community acquired UTI as the source of their BSI. On one side there seems te be a culture of overtreatment of UTI (a clinical diagnosis) in Belgium which in fact are not UTI, and on the other side there seems to be a gap in reliable clinical judgment in primary care in cases of life threatening infections (the classical signs of septicaemia are not recognized).
Antibiotic stewardship could also help and fosfomycin PO seems to be the best choice now for treating UTI outside the hospital in Belgium.
LikeLike
Today I had interesting discussions with some knowledgable colleagues from the future Brexit Kingdom (names available upon request). I learned that the observed increase of E. coli BSI is real and impressive, but also fully unexplained yet. One of them also feared that my first solution (stop taking blood cultures in sepsis) would become popular. In order to avoid that scenario, we realized that it is actually not needed. Here is solution 4: in a septic patient reverse the order of taking a blood culture before giving the antibiotic.
Sounds silly, but all I want to say is that this ambition, once transfered into a quality indicator will change things that we – as concerned professionals – may not want to change. Is there a plan to prevent that?
LikeLike
Firstly the ambition is to halve healthcare associated GNBSI not all; so that is about a 25% reduction for E. Coli and based on the Fitzpatrick et al paper probably 75% of Klebsiella and Pseudomonas (more traditional hospital onset infection pathogens).
So we monitor the total number of blood cultures taken in England quarterly and these are also published on the PHE AMR Indicators pages. Similar arguments were made for MRSA and also with stool samples with CDI, but that was not the prime reason for the reductions.
I think this will be difficult but if it focuses hearts and minds, stops further increases, improves diagnosis and treatment of UTIs in the community and reduces CAUTI and colorectal SSI, then it will still have been successful!
LikeLike
I think the issue of poorly managed, clear cut, acute UTIs as a cause of sepsis in the community is just not true. What is true is that we have an ageing population with multiple comorbidities and the interventions that are likely to work (that Martin describes) are just not on the infection control radar. Plus, there is no single chief exec whose job will be on the line. Responsibility is too diffuse. I think we need to invent community infection services. But infection control does not necessarily have a good name in primary care. Seen as busy bodies worrying about trivial things in doctors surgeries, while ignoring the complex but important stuff that’s going on in the black hole of care homes. Where is public health in leading this debate? Or more importantly, buying the interventions, and perhaps providing the accountability, rather than complaining about everyone elses failings.
LikeLike