A really important point prevalence survey of CPE carriage in inpatients in a hospital in Manchester has just been published in the Journal of Hospital Infection. Important because of the high rate of carriage (11% of 662 patients included). Important because for every 1.6 known cases of CPE, there was an undetected case lurking, despite an extensive screening programme. Important because the lack of significant risk factors associated with CPE carriage suggests that it is distributed homogeneously, endemic in the population. And important because this is the first citable publication suggesting that Manchester has a problem with CPE, despite us having known about it for years via professional networks.
This is an extensive point prevalence screening programme, which aimed to screen all inpatients who were not already known carriers of CPE over a 3 day period. They achieve impressive coverage of the inpatient population, screening 623 (89%) of 703 eligible patients. It’s great to see such a high rate of screening acceptance from both a staff and patient viewpoint.
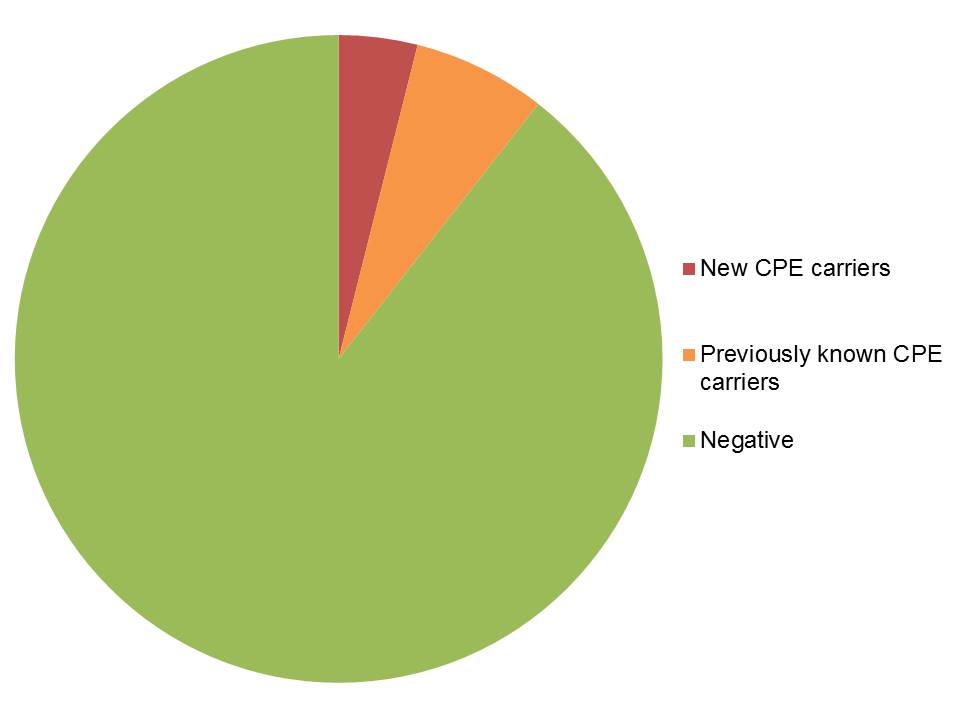
A whopping 11% of 662 patients were carrying CPE (26 newly identified and 44 previously known (see Figure). This suggests that the extensive admission and weekly screening programme was not detecting CPE carriers effectively. There’s one beautifully academic statement in the discussion: ‘The prevalence of CPE at CMFT is likely to be higher than other settings in the UK’; I’d be amazed if it wasn’t! I don’t want this blog to be misinterpreted: there’s no intended criticism of colleagues in Manchester. This could have happened (and indeed could be happening) to any of us working in healthcare. I’m just delighted to see some data from Manchester being published
Figure: CPE carriage status in the 662 patients included in the point prevalence survey.
PCR was used as a front-line test, with samples positive by PCR cultured in an attempt to grow the CPE. For 7 (27%) of samples positive by PCR, no CPE could be grown. This suggests that PCR is more sensitive in detecting CPE, although the possibility of carbapenemase genes in non-Enterobacteriaceae (such as Acinetobacter), and the slim possibility of a misfiring PCR assay that lacks specificity can’t be ruled out.
The prevalence of CPE carriage was the same in each of the clinical divisions (Medicine, Surgery, Specialist Medicine, and Critical Care). If this was an emerging problem, you’d expect the rate of carriage to be higher in one of these areas. Also, although a few risk factors were associated with CPE carriage in univariable analysis, no risk factors were associated with CPE carriage in a multivariable analysis. A high proportion of the CPE identified were KPC (88%), and the majority of patients (both CPE positive and negative) were of white, British ethnicity. Whilst it could be that the study was underpowered to detect statistically significant risk factors (and I’m not sure why the previously known cases were not included in the analysis), taken together, these findings suggest that CPE is already distributed homogeneously and thoroughly endemic in this hospital.
This study is deeply concerning, and illustrates how quickly CPE can become established in a hospital population. It’s difficult to see how this situation can be recovered, although there are some encouraging success stories in reversing seemingly dire CPE situations.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
