The Mpox outbreak in the Democratic Republic of Congo (DRC) continues, with the latest estimates suggesting that there have been >25,000 cases and >700 deaths since the beginning of 2023. There have been three cases of confirmed Clade Ib Mpox reported in the UK in the past week. I posted recently with some background info on the epi of Mpox. Today’s post is based on an epi modelling study exploring key epidemiological parameters of Clade I Mpox based on historical data to inform our understanding of the Clade Ib outbreak: the incubation period, serial interval, generation interval, and reproduction number. There will be an IPC Partners Journal Club on this study next week on Weds 13th November (register here).
To understand the study, we need to understand what these epidemiological parameters mean and how they differ. Figure one gives a graphical explanation of the incubation period, serial interval, and generation interval.
Figure 1: Graphical illustration of the incubation period, serial interval, and generation interval (from Zhao et al.)
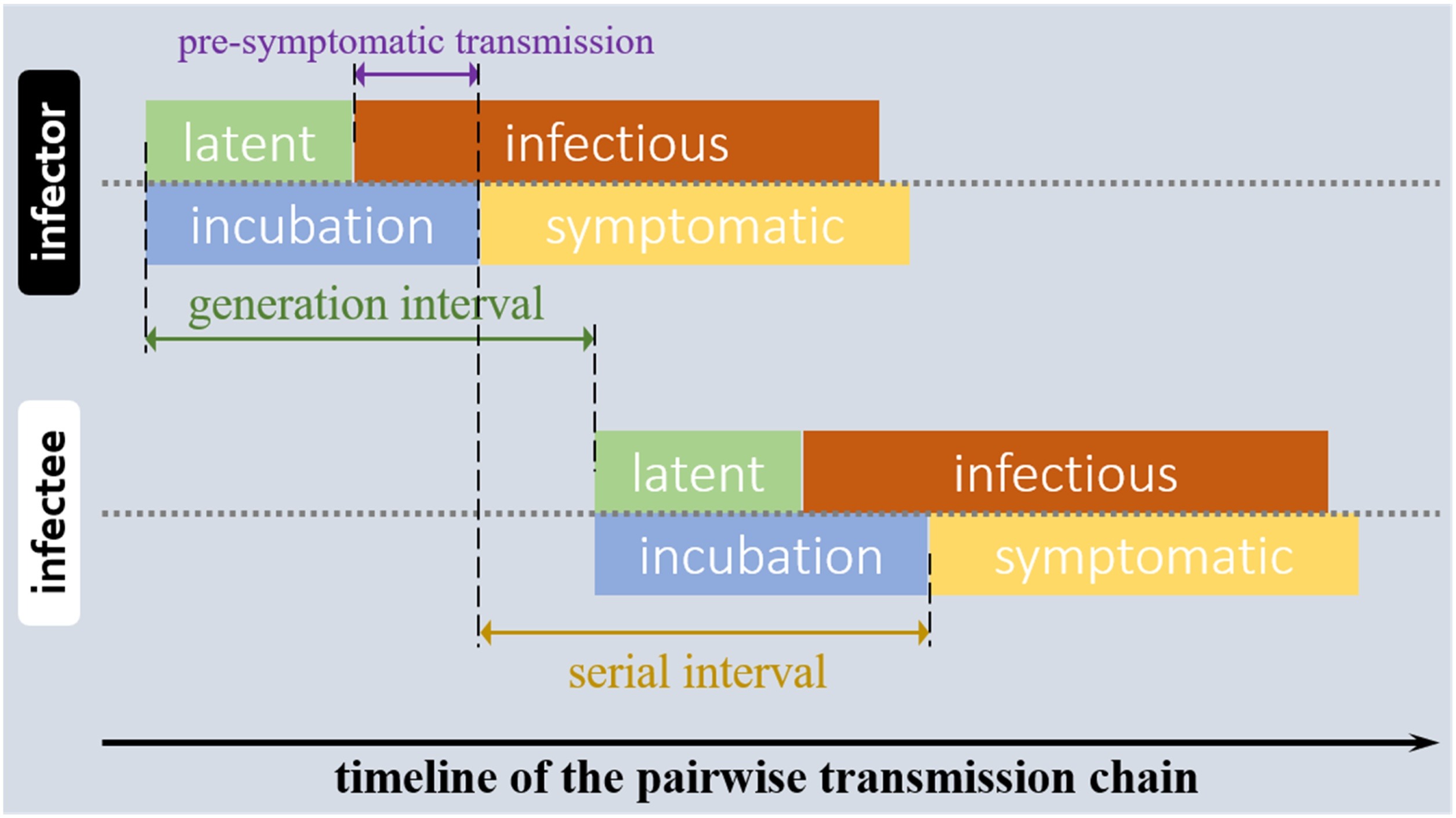
As you can see, these parameters are somewhat overlapping – and because of this overlap, we are able to make some inferences on the likely contribution of pre-symptomatic transmission.
R0, or the basic reproduction number, is a figure expressing the average number of cases of an infectious disease arising by transmission from a single infected individual, in a population that has not previously encountered the disease. A closely related metric is the time-varying reproduction number Rt, which represents transmissibility over time.
The incubation period was estimated using data from 15 patients with sufficient detail on disease onset. Serial interval and generation interval were estimated from two datasets, one with 32 household transmission infector / infectee pairs, and one with 11 hospital transmission infector / infectee pairs from a single hospital outbreak in DRC.
Key findings:
- Incubation period (mean): 9.9 days.
- Serial interval (mean): 17.5 days for household transmission and 11.4 days for hospital transmission.
- Generation interval (mean): 17.2 days for household transmission and 11.3 days for hospital transmission.
- Three different epidemiological methods were used to estimate these parameters, all of which yielded comparable results.
- Pre-symptomatic transmission was felt to play a minor role, accounting for <20% of transmissions.
- The mean Rt for the 2024 outbreak in DRC was estimated to be <1 overall, but >1 for one DRC region (Kamituga). A possible reason for this difference is a higher concentration of sex workers in this region.
Some points for discussion:
- The estimate of incubation period falls within the commonly cited range of 5-21 days.
- Mpox is transmitted via a variety of routes, but most commonly very close physical (and often sexual) contact. The hypothesis that the slightly higher Rt in Kamituga is explained by a higher concentration of sex workers in the region reinforces the role of sexual contact in the spread of Mpox.
- Taken together, the epidemiological parameters estimated in this study from historic Clade I data present an infectious disease with low transmissibility compared with others. For example, in this study, Rt was hovering just above or just below 1. By way of companion, reproduction numbers for measles are probably in the high 10s of even 100s for measles and in the 10s for chickenpox, and between 1 and 3 for Clade IIb Mpox.
- The datasets used as a basis for estimating these epidemiological parameters are limited. For example, the information on serial intervention and generation interval in hospitals is based on 11 infector / infectee pairs from an outbreak in one hospital. A dataset including a wider variety of settings and scenarios would make the estimates more generalisable.
- One challenge when estimating transmission parameters is incomplete surveillance, which is often limited by diagnostic capability. This influence estimates of R in particular, because if secondary cases are missed, then R is underestimated.
So, will Clade Ib Mpox be the next pandemic? Compared with other infectious diseases, the transmissibility of Mpox is low – and linked to very close physical contact. Whilst Mpox Clade IIb has caused issues across the globe, this has remained almost exclusively within a defined population (gay, bisexual, and other men who have sex with men) and has not resulted in widespread community transmission. Risk assessments undertaken by public health agencies concludes that the risk to the general population from Mpox of any clade remains low (e.g. ECDC). Therefore, it seems very unlikely that Mpox Clade Ib will be the next pandemic (but never say never)!
Finally, there will be an IPC Partners Journal Club on this study on Weds 13th November (register here). If you haven’t been to an IPC Partners Journal Club before, the format is a short introduction of the paper followed by Q&A from the audience. They are scheduled at 1000 EST / 1500 GMT (UK) to facilitate live participation from those in North America and Europe. Journal Club recordings are available here for those who aren’t able to join live.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
