There has been a huge amount of debate, discussion (and occasional vitriol) about transmission routes for respiratory pathogens, especially SARS-CoV-2. One of the sticking points has been different perspectives on the terminology used. I was privileged to join a working group convened by WHO to propose some new terminology to underpin this discussion. The proposed new terminology has been published recently, and I’d thought I’d share some reflections! Whilst I don’t think this will turn our IPC practice upside down, it is a step towards a more informed approach to preventing the spread of respiratory pathogens.
Three women walked into a bar before the pandemic. An engineer, a microbiologist, and a member of the public. If you asked them all to describe what they meant by the terms “aerosol”, “droplet”, and “airborne”, you’d get at least three different answers for each. (Whilst this might have started like a joke, I’m sorry to say that this is the closest you’re going to get to a punchline.) A nice article by Julian Tang and colleagues published fairly early in the pandemic illustrated this point.
The aim of the group therefore was to bring together a multiprofessional group to come up with some consensus terminology to describe this issue accurately and in a way that would make sense to the people who need to put this terminology into action. It would have been no good coming up with very accurate but clunky terms that nobody would end up using (and you could argue that “Through the air” falls into this category).
New terms
So, what new terms does this consensus document bring into our vernacular?
- “Through the air” – a catch-all term to describe any transmission that occurs with the air as a vector. In ‘old money’, this would include both “droplet” and “airborne” routes. A parallel term to “foodborne” or “waterborne”.
- “Infectious particles” – pathogens contained within a particle.
- “Infectious respiratory particles (IRP)” – pathogens contained within a particle that are carried by expired airflow.
- “Puff cloud” – the jumble of particles that are expired by humans.
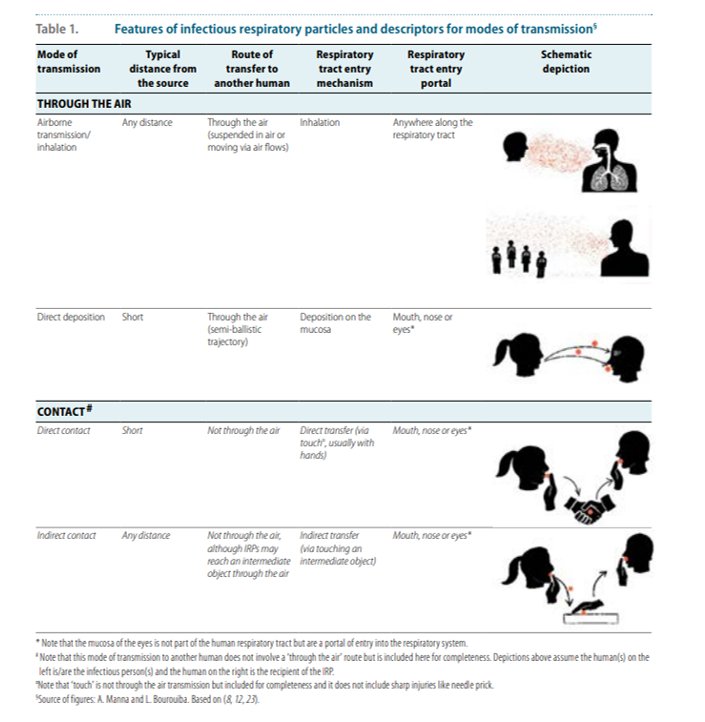
- “Airborne transmission / inhalation” – the transmission of an IRP from one person to another via inhalation at any point into the respiratory tract, which can occur over short or long distances. This is roughly analogous to the “old” idea of “airborne transmission”.
- “Direct deposition” – the transmission of an IRP from one person to another via direct deposition on exposed facial mucosal surfaces (i.e. mouth, nose, eyes) following a short range semi-ballistic trajectory. This is analogous to the “old” idea of “droplet transmission”.
The story of the consensus paper is best told by the two images below – the first of which provides a schematic overview of potential through the air modes of transmission, and the second provides a framework for understanding the various modes of through the air transmission.
Figure: schematic overview of potential through the air modes of transmission

Points for discussion
- There were several points that, as I’m sure you are not surprised to hear, prompted much discussion and debate. I don’t agree with where every part of this consensus document landed. And I’m sure that’s true of every member of the group. But I do think it’s a useful consensus document, that takes this discussion forwards in a useful direction. Some of the points of disagreement are outlined in Annex 5 of the consensus document.
- There was extended debate about what the “catch-all” term for “Through the air” transmission should be, with some arguing that this should be “Airborne” (to align with “Foodborne” and “Waterborne”) and others arguing that “airborne” should be reserved as a term linked to inhalation.
- There has always been a “false dichotomy” based on arbitrary particle size cut off between large droplets that don’t travel far or stay in the air for long, and aerosols that can travel a long way and remain suspended in the air for the long time. This consensus document puts this issue to bed, stating clearly that there is no useful binary distinction between “large” droplets and “small” aerosols – but rather a continuum of particle size.
- Despite this continuum in particle size, the document retains a practical distinction between “Airborne transmission / inhalation” and “Direct deposition”.
- There was much discussion on the difference between “exposure” (i.e. where an IRP makes it from person A, the source, to person B, the susceptible host) and “transmission” (i.e. where an IRP makes it from person A to person B, and overcomes a variety of environmental, host, and microbial factors to replicate and initiate an infection). One aspect of this that requires more discussion is infectious dose – looking at the literature, the infectious dose to initiate infection is often rather high. To some, exposure is synonymous with transmission. Whereas to others (me included!), there is an important distinction to be drawn between exposure and transmission. If our aim is to prevent exposure, then our approach and interventions will be different than if our aim is to prevent transmission. The consensus document concludes clearly that our aim should be to prevent transmission, and not all exposure: ‘There must be a clear understanding that when describing transmission of pathogens, this must work backwards from factors affecting infection risk, not just forwards from source generation and infectious particle characteristics, such as their concentrations, size and aerobiological properties.’
Implications
The terminology proposed in the consensus document maps neatly into the current approach to transmission-based precautions as outlined in the National Infection Prevention and Control Manual. Airborne Precautions would be applied to prevent “Airborne transmission / inhalation” and Droplet Precautions would be applied to prevent transmission via “Direct deposition”. There is still clearly the open and rather complex question of when to apply which set of precautions in various scenarios!
Finally, thanks to WHO for convening this group, and for bringing us to a consensus.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
