This is a guest post by the marvelous Jude Robinson (bio below) for some work that she has co-led with Emma Burnett…
I had the pleasure to present our completed study findings of the IPS designing an optimal infection prevention and control service (DOIPS) study at the recent Infection Prevention 2022 conference. This is a four phased- mixed method study which began late in 2017, and was completed in the autumn of 2021.
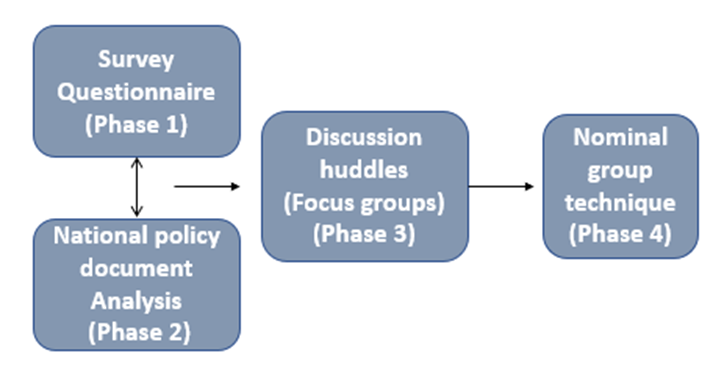
Figure 1: Methods
We surveyed the Infection Prevention Society (IPS) workforce in 2018, and for the first time, this provided a snapshot of what the IPC workforce looked like in relation to demographics such as job titles, staff numbers, skill mix, budgets, services covered and core components, vacancies, and education. A policy document analysis carried out in 2018 by Evonne Curran highlighted that the current IPC priorities needed simplifying. At the time, it was felt that IPC importance had been downgraded, and Evonne questioned whether IPC priorities were in the right place and acknowledged the need for a more effective collaboration between national authorities. The third phase of the study saw 5 discussion huddles undertaken between 2018-2019, involving 53 participants. This phase really enabled us to explore a rich narrative and gain more insight to some of the answers we received in the first two phases of this study, and we were able to focus on the core components of the current IPC workforce. At the time, no single priority was identified, but rather there were several key components interlinked for an effective IPC service. Barriers and facilitators to the success of an IPC service were explored in detail and further details can be found in this study.
The fourth and final phase of this study was a consensus method called a modified nominal group technique (NGT). This was structured face -to-face group discussions with the aim of achieving a group consensus on two specific questions. This took place at the IP2021 national conference in the format of a workshop. The two topic questions that were asked were;
1: What are the key priorities for an IPC service?
2: What are the key enables for success?
These two topic questions were asked with the aim to consolidate the three previous phases and help us to answer the overall research question which was to define an optimal IPC service in different contexts and settings within the United Kingdom and Ireland.
These topic questions were then presented to 39 IPC professionals, from a variety of roles, ranks and expertise who attended the workshop. The 39 staff were split into 3 smaller groups with each group being facilitated by one of the research team. Each group followed the same process at exactly the same time.
- The first stage was to gain individual responses to the topic questions. This was a 15-minute period of silence, where each participant was asked to write responses to the topic question. Each individual response was scribed on a post-it-note until the dedicated time had lapsed. The number of responses per participant varied.
- The next stage was a 20–25-minute period where each participant was asked to state what they had written on each post-it-note. Each participant took it in turns to say one response at a time, until everyone had said all of their responses from their post-it-notes. During this time, if a response needed clarification, then we discussed this in our small groups. If a response had already been said, then this was not added to the list.
This was then repeated for the second topic question. At the end of this face-to face session, we had 3 large flip chart paper full of responses for each of the two topic questions.
The final stage of the NGT was to rank responses until a consensus is achieved, but before we could do that, we had to consolidate the 3 separate groups responses into one list of responses. This was carried out by two members of the research team.
We were overwhelmed with the number of responses for each topic question, with a total of 45 responses for key priorities and 69 responses for key enablers. Due to the high number of responses, we knew that we would not get through this ranking in the time allocated for the second planned workshop at the IP2021 conference, so the ranking was carried out virtually.
Each participant was sent a PowerPoint presentation with all the responses listed along with a ranking form, where each response needed to be ranked between 5 and 1 (5 extremely important, 4 very important, 3 important, 2 somewhat important and 1 not important at all). This was emailed to each participant.
24 participants returned their ranking forms. The highest a response could have ranked was a total of 120 points (24 × 5 = 120). The lowest a response could have ranked was a total of 24 points (24 × 1 = 24). There were several responses that reached the same score for each of the topic questions. The full ranked responses can be found here.
Here, we share with you the top five priorities and top five enablers, and you can see that we have captured the responses that scored equally as part of this.
The top 5 key priorities for an effective service are;
- Preventing HCAI to persevere patient safety
- Engagement of frontline staff and Embedding Key IPC Principles into practice
- Education of the IPC team
- Evidence based practice
- Effective outbreak management and Resource- IPC staffing to enable realistic workload and Effective leadership all levels
The top five enablers for success are:
- Adequate staff resources
- Appropriate, flexible, realistic and evidence based national standards/guidelines and a trained, competent IPC team
- IPC commitment at board level
- Adequate funding
- Visibility of IPC team within the organisation and effective communication and staff well-being and morale
From this ranking of key priorities and enablers we are really excited to present a conceptual model for designing an optimal infection prevention service, which can be used to develop IPC services at a local, regional, national, and hopefully international level. This has received some peer review from NHE England and an international IPC expert from the world health organisation.

Figure 2: Conceptual model for designing an optimal IPC service.
This framework was deliberately conceptual, as one of the core objectives of this study was to define an optimal IPC service in different contexts and settings. We didn’t want a framework that would only work for acute settings or just for community, it needed to work for all IPC services and settings.
We have matrixed this against the WHO core component (hyperlink to WHO core components) to ensure it has a global connection.
We decided to use the top key priority as the main driver, and then we have 4 streams as themed enablers, and then we have several elements within each of the themed enablers.
As a summary, when we look broadly at what an IPC workforce should look like, it has got to be a workforce where the health and wellbeing of IPC staff is prioritised. I may be bold when I say this, but I think IPC is a broken workforce where staff have been pushed to limits that we never thought was possible during the pandemic, so we need to protect them and look after them. We need highly specialist teams who intelligently use data to respond and adapt to local needs. We need an IPC workforce that uses evidence-based policies and education for the healthcare system it serves and where IPC teams are integrated into the whole healthcare management structure.
We have presented this conceptual framework at IP2022 where this was well received, and we were able to gain some feedback on this too. We now need a focus around the implementation of this conceptual framework, so the highlighted enablers are effectively embedded into IPC services and wider healthcare settings.
Bio
Jude Robinson is an Infection Prevention and Control Senior Manager for NHS England- Midlands region. Jude has been working within the field of infection prevention and control for 14 years, where she has held a variety of clinical and academic roles.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
