A guest post by Professor Sally Bloomfield explores whether we are over-emphasizing the role of hand washing in preventing the spread of infection…
If you ask whether I think hand hygiene is the single most important intervention for preventing spread of infection, I would answer yes. But I also think the COVID pandemic requires us to re-evaluate how we look at infection prevention (or hygiene) to make it relevant to the issues we now face, which are as much about “airborne “ transmission routes as hands and contact surfaces.
At the outset, the prevailing belief was that Covid-19 was primarily transmitted through droplets, through skin-on-skin contact, such as shaking hands, being coughed on by an infected person or touching something they had recently touched. The messaging was hands, space, face – in that order. But by placing them in that order it fostered the idea that handwashing was the MOST important. Was that intentional?
We now recognise that, for SARS-CoV-2, “airborne” transmission, involving small aerosol particles that travel significant distances and are inhaled, is likely to be the main transmission route, and the “message” has been modified to include face coverings and ventilation as well as hands and space.
In recent months, however, there have been media articles about “How excessive cleaning gives us a false sense of security” and “Why I’m cutting back on hand washing (but keeping my mask on)”. Although modelling studies suggest that “contact transmission” could be responsible for up to 30 % of COVID-19 cases, the validity of the data is challenged by some who believe that the risk from contact surfaces is “vanishingly small” and that “we should double down on the tried and tested hygiene practice of handwashing. Everything else is irrelevant,”. But – if we are no longer shaking hands with each other, hands are only a risk if we touch a surface recently contaminated by someone else – we cannot separate the two?
Maybe we have strongly prioritised hand hygiene in recent years, but not without cause. The last 50 years have seen significant investment in getting healthcare professionals to wash their hands in order to protect patients – and importantly the development of “my 5 moments for hand hygiene” to enable us to target the critical moments when this is needed. Equally, in low and middle income communities (LMICs) across the world, whereas prior to 2000 the emphasis was on provision of water and sanitation, since 1980s we have seen this expand to include hygiene – and the development of WASH. But, although WASH stands for Water, Sanitation and Hygiene, to NGOs and healthcare workers in these regions, in reality hygiene means handwashing. Focusing on hand hygiene is justified because the evidence indicates it gives us the biggest bang for our bucks in terms of reducing nosocomial infection and the global burden of diarrhoeal disease in LMICs.
But, downplaying hand and surface hygiene is dangerous in a world where the public want to polarise actions into “safe” or “unsafe” i.e they want to know which actions will 100% make them safe and which do not, and can be abandoned. This concern prompted pieces in The Conversation and Guardian pointing out the vital role of hand hygiene in the global fight against infectious and tackling AMR by reducing the need for antibiotic prescribing.
Perhaps it is time to consider whether one of the barriers to progress is a failure to realise that prevention of infection, i.e hygiene, is not a clinical issue, it’s about risk management – and needs to be addressed as such. i.e. hand hygiene is not a discreet intervention, but one of a set of interdependent critical control points where intervention is necessary at “moments” when there is risk of spread on infection.
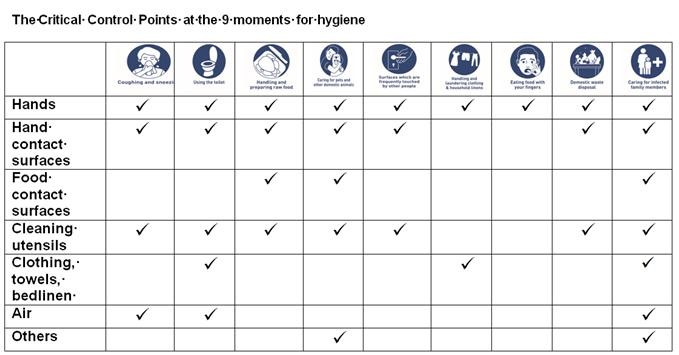
Since 1997, the IFH has used this approach to develop hygiene for home and everyday life settings. It recognises that the main sources of the infectious microbes in any indoor setting are people, contaminated food and domestic animals. From this, we have identified 9 key moments in our daily lives (handling food, using the toilet etc) where we carry out activities that cause these microbes to spread. These are the moments when we need to practise hygiene. The bottom line is – if we are not exposed to harmful microbes we can’t be infected.
A key concept of Targeted Hygiene is that, at each key moment, hygiene practices must be carried out at ALL critical points. The “Swiss cheese model” shows how barriers of protection work together to minimise the risk of infection.
One of the 9 key moments for hygiene (and the one relevant to COVID-19) is “coughing, sneezing or nose blowing (also when singing or talking loudly in a closed environment)”. At this moment i.e. during these activities, critical control points are the hands, hand contact surfaces, and air. Although only a small number of people may be infected via hands and surfaces compared to airborne routes, because it is unpredictable who they will be, risk management means that we ALL practise hand and contact surface hygiene as well as wearing face masks and social distancing. In a population of 65 million people, actions considered as relatively lower risk contribute significantly to the overall disease burden. It demonstrates why control points must not be abandoned because they are less important than others. The wearing of masks is a case in point.
Importantly, Fig 1 shows that, hand hygiene is central to ALL of the 9 key moments, but needs to be combined with interventions at other interdependent control points to ensure that the risk is contained. Adopting this relatively simple approach, gives us a realistic chance of changing public perceptions, by using visual images of each key moment as prompts for action (rather than trying to memorise a list), and of the critical actions needed to prevent spread at each moment.
A public poll carried out in 2020 suggests that a key barrier to behaviour change is public misunderstanding of hygiene. The poll suggests that the public still tend to believe that dirt is the main source of harmful microbes and that regular cleaning and disinfection is the answer. This rooted obsession with dirt and germs is demonstrated by the images of public health workers spraying “non contact” surfaces in open public spaces, and deep cleaning indoor premises, in the mistaken belief that it makes them COVID secure. The confusion is not just with the public. Government advice that we should “wash your hand frequently and thoroughly” misses the point that the public need to know “when” to wash hands.
Hand hygiene at risk moments is a cost-effective, proven method of suppressing infection in all settings worldwide, and has the potential if correctly applied to control the whole spectrum of pathogenic microbes. It is vital that we embed societal hygiene understanding and appropriate hygiene behaviours, so that we are prepared for public health issues we face ongoing. Since our understanding of hygiene is built on early home experience, hygiene literacy would also form the basis of better understanding of infection prevention in our professional lives in healthcare and other settings.
Discover more from Reflections on Infection Prevention and Control
Subscribe to get the latest posts sent to your email.
